Department of Anesthesiology and Reanimation, Faculty of Medicine and Health Sciences, Sherbrooke University Hospital, Sherbrooke, Québec, Canada.
Department of Anesthesiology and Reanimation, Faculty of Medicine and Health Sciences, Sherbrooke University Hospital, Sherbrooke, Québec, Canada.
Nutrition. 2019 May;61:84-92. doi: 10.1016/j.nut.2018.10.026. Epub 2018 Nov 5.
Acute respiratory distress syndrome (ARDS) is characterized by an acute inflammatory response in the lung parenchyma leading to severe hypoxemia. Because of its anti-inflammatory and immunomodulatory properties, omega-3 polyunsaturated fatty acids (ω-3 PUFA) have been administered to ARDS patients, mostly by the enteral route, as immune-enhancing diets with eicosapentaenoic acid, γ-linolenic acid, and antioxidants. However, clinical benefits of ω-3 PUFAs in ARDS patients remain unclear because clinical trials have found conflicting results. Considering the most recent randomized controlled trials (RCTs) and recent change in administration strategies, the aim of this updated systematic review and meta-analysis was to evaluate clinical benefits of ω-3 PUFA administration on gas exchange and clinical outcomes in ARDS patients.
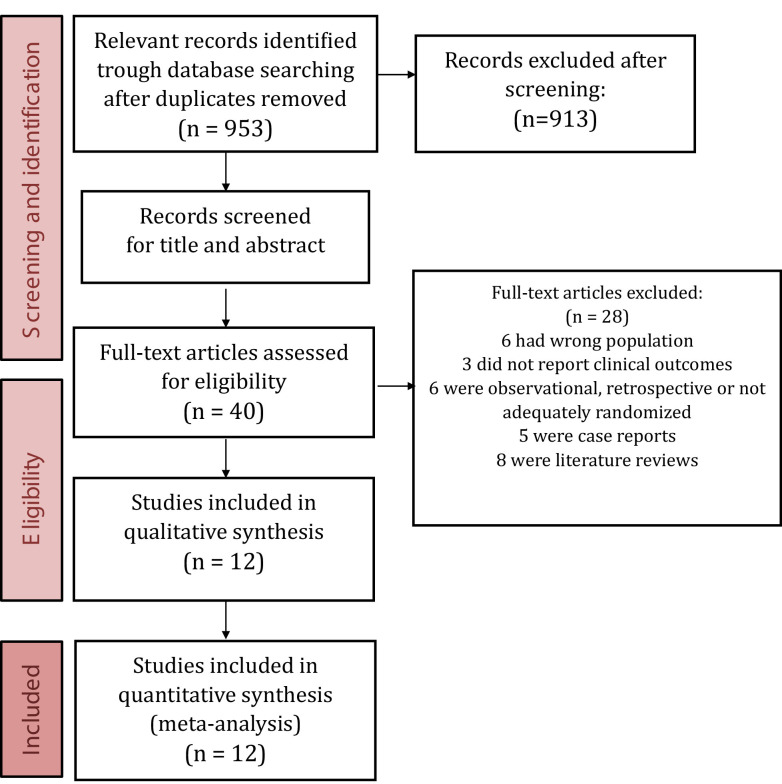
We searched for RCTs conducted in intensive care unit (ICU) patients with ARDS comparing the administration of ω-3 PUFAs to placebo. The outcomes assessed were PaO-to-FiO ratio evaluated early (3-4 d) and later (7-8 d), mortality, ICU and hospital length of stay (LOS), length of mechanical ventilation (MV), and infectious complications. Two independent reviewers assessed eligibility, risk of bias, and abstracted data. Data were pooled using a random effect model to estimate the relative risk or weighted mean difference (WMD).
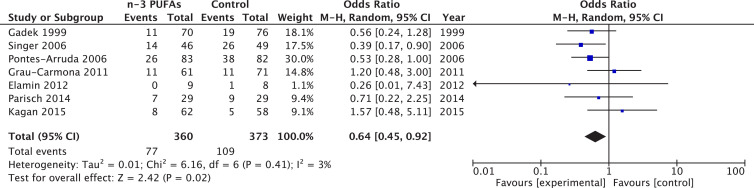
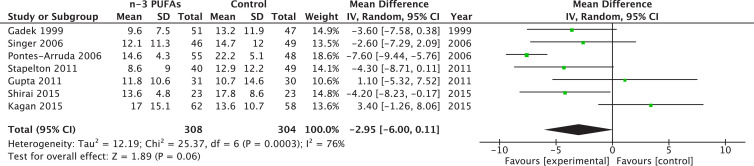
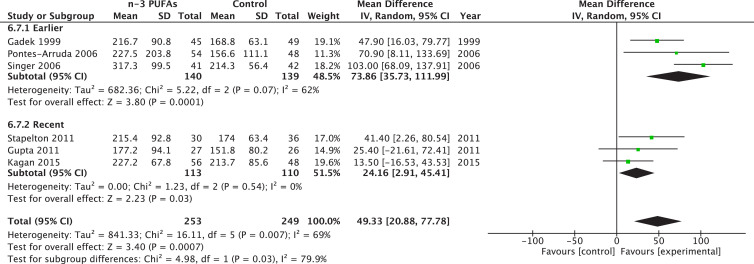
Twelve RCTs (n = 1280 patients) met our inclusion criteria. Omega-3 PUFAs administration was associated with a significant improvement in early PaO-to-FiO ratio (WMD = 49.33; 95% confidence interval [CI] 20.88-77.78; P = 0.0007; I = 69%), which persisted at days 7 to 8 (WMD = 27.87; 95% CI 0.75-54.99; P = 0.04; I = 57%). There was a trend in those receiving ω-3 PUFA toward reduced ICU LOS (P = 0.08) and duration of MV (P = 0.06), whereas mortality, hospital LOS, and infectious complications remained unchanged. Continuous enteral infusion was associated with reduced mortality (P = 0.02), whereas analysis restricted to enteral administration either with or without bolus found improved early PaO and FiO (P = 0.001) and MV duration (P = 0.03). Trials at higher risk of bias had a significant reduction in mortality (P = 0.04), and improvement in late PaO-to-FiO ratio (P = 0.003).
In critically ill patients with ARDS, ω-3 PUFAs in enteral immunomodulatory diets may be associated with an improvement in early and late PaO-to-FiO ratio, and statistical trends exist for an improved ICU LOS and MV duration. Considering these results, administering ω-3 PUFAs appears a reasonable strategy in ARDS.
急性呼吸窘迫综合征(ARDS)的特征是肺部实质的急性炎症反应,导致严重的低氧血症。由于其抗炎和免疫调节特性,ω-3 多不饱和脂肪酸(ω-3 PUFA)已被用于 ARDS 患者,主要通过肠内途径,作为具有二十碳五烯酸、γ-亚麻酸和抗氧化剂的免疫增强饮食。然而,ω-3 PUFAs 在 ARDS 患者中的临床益处仍不清楚,因为临床试验得出了相互矛盾的结果。考虑到最近的随机对照试验(RCT)和最近的给药策略的改变,本更新的系统评价和荟萃分析的目的是评估 ω-3 PUFA 给药对 ARDS 患者气体交换和临床结局的临床益处。
我们搜索了在 ICU 中患有 ARDS 的患者中进行的 RCT,比较了 ω-3 PUFAs 与安慰剂的给药。评估的结局包括早期(3-4 天)和晚期(7-8 天)的 PaO 与 FiO 比值、死亡率、ICU 和住院时间(LOS)、机械通气(MV)时间和感染并发症。两名独立的审查员评估了合格性、偏倚风险和摘要数据。使用随机效应模型汇总数据以估计相对风险或加权均数差(WMD)。
12 项 RCT(n=1280 名患者)符合我们的纳入标准。ω-3 PUFAs 给药与早期 PaO 与 FiO 比值的显著改善相关(WMD=49.33;95%置信区间[CI]20.88-77.78;P=0.0007;I=69%),这一比值在第 7 至 8 天仍然存在(WMD=27.87;95%CI 0.75-54.99;P=0.04;I=57%)。接受 ω-3 PUFA 的患者 ICU LOS (P=0.08)和 MV 时间(P=0.06)有下降趋势,而死亡率、住院 LOS 和感染并发症没有变化。连续肠内输注与死亡率降低相关(P=0.02),而仅在肠内给予或不给予冲击剂量的分析发现,早期 PaO 和 FiO 改善(P=0.001)和 MV 时间缩短(P=0.03)。高偏倚风险的试验死亡率显著降低(P=0.04),晚期 PaO 与 FiO 比值也得到改善(P=0.003)。
在患有 ARDS 的危重病患者中,肠内免疫调节饮食中的 ω-3 PUFAs 可能与早期和晚期 PaO 与 FiO 比值的改善相关,并且 ICU LOS 和 MV 时间的改善存在统计学趋势。考虑到这些结果,给予 ω-3 PUFAs 似乎是 ARDS 的一种合理策略。