The World Bank Group, Washington, District of Columbia, USA.
IPAS, Chapel Hill, North Carolina, USA.
BMJ Open. 2019 Jan 30;9(1):e023021. doi: 10.1136/bmjopen-2018-023021.
To quantify sex ratios at births (SRBs) in hospital deliveries in Nepal, and understand the socio-demographic correlates of skewed SRB. Skewed SRBs in hospitals could be explained by sex selective abortion, and/or by decision to have a son delivered in a hospital-increased in -utero investments for male fetus. We use data on ultrasound use to quantify links between prenatal knowledge of sex, parity and skewed SRBs.
Secondary analysis of: (1) de-identified data from a randomizedrandomised controlled trial, and (2) 2011 Nepal Demographic and Health Survey (NDHS).
Nepal.
(1) 75 428 women who gave birth in study hospitals, (2) NDHS: 12 674 women aged 15-49 years.
SRB, and conditional SRB of a second child given first born male or female were calculated.
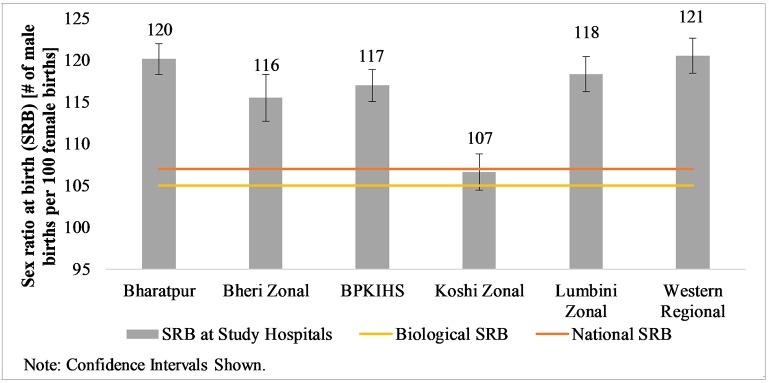
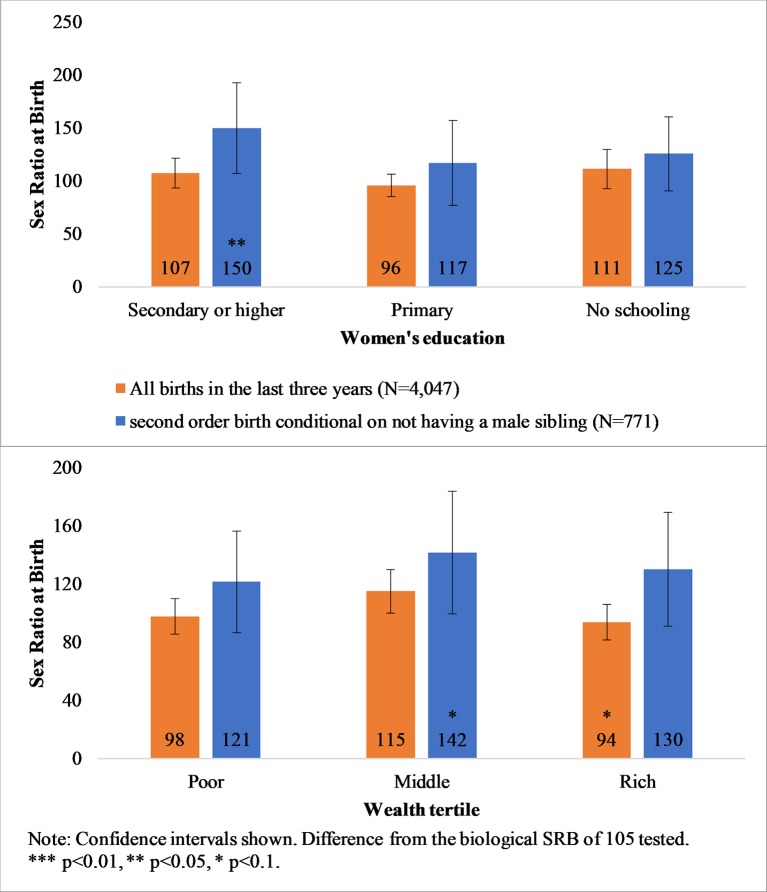
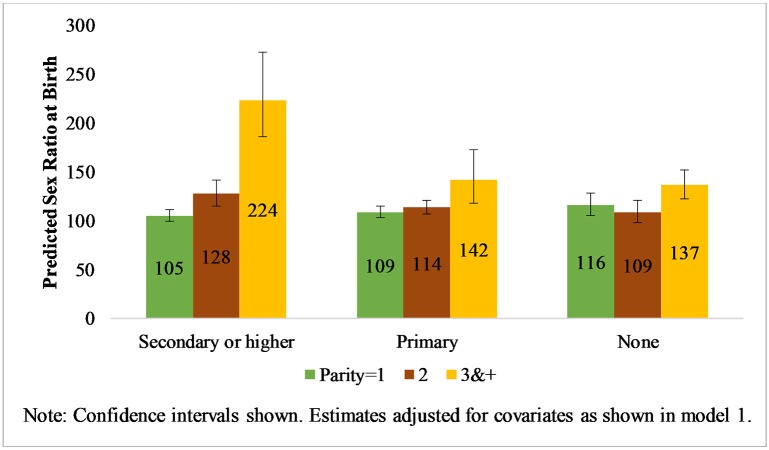
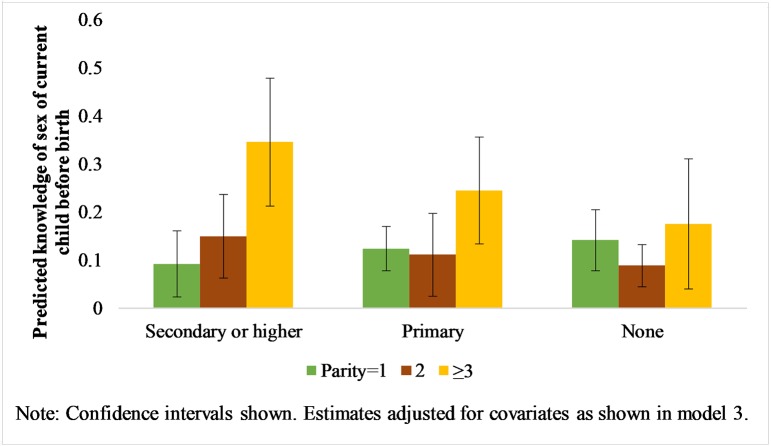
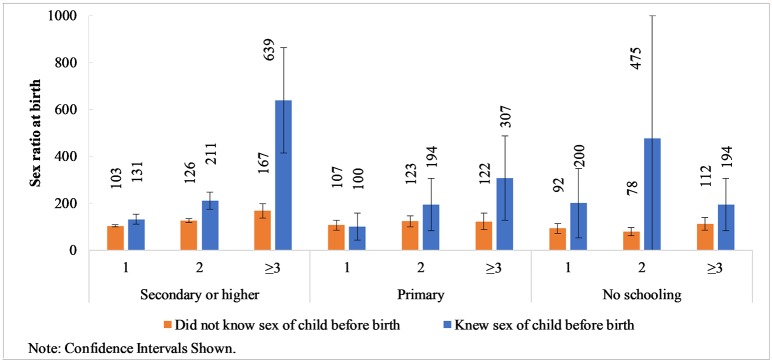
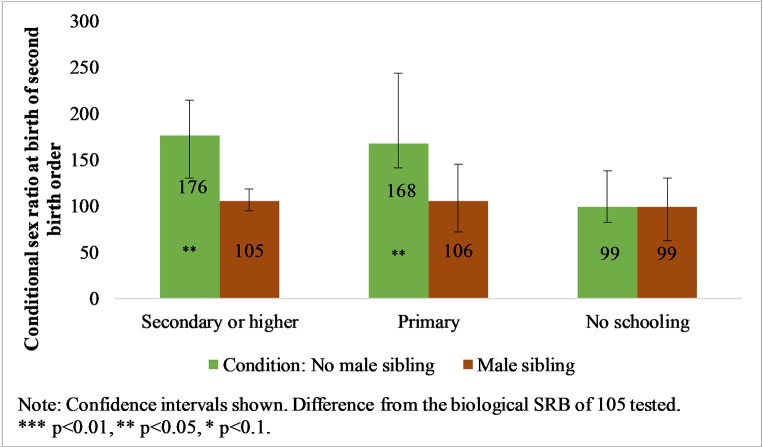
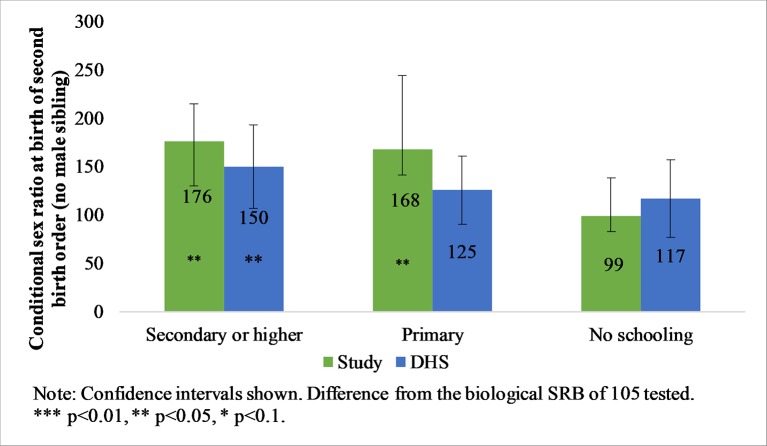
Using data from 75 428 women who gave birth in six tertiary hospitals in Nepal between September 2015 and March 2017, we report skewed SRBs in these hospitals, with some hospitals registering deliveries of 121 male births per 100 female births. We find that a nationally representative survey (2011 NDHS) reveals no difference in the number of hospital delivery of male and female babies. Additionally, we find that: (1) estimated SRB of second-order births conditional on the first being a girl is significantly higher than the biological SRB in our study and (2) multiparous women are more likely to have prenatal knowledge of the sex of their fetus and to have male births than primiparous women with the differences increasing with increasing levels of education.
Our analysis supports sex-selective abortion as the dominant cause of skewed SRBs in study hospitals. Comprehensive national policies that not only plan and enforce regulations against gender-biased abortions and, but also ameliorate the marginalizedmarginalised status of women in Nepal are urgently required to change this alarming manifestation of son preference.
NCT02718222.
量化尼泊尔医院分娩中的出生性别比(SRB),并了解出生性别比偏斜的社会人口学相关因素。医院中出生性别比偏斜可能是由性别选择性堕胎引起的,也可能是由于决定在医院分娩男孩导致对男性胎儿的宫内投资增加。我们利用超声使用数据来量化产前性别知识、生育次数与出生性别比偏斜之间的关系。
对(1)随机对照试验的匿名数据和(2)2011 年尼泊尔人口与健康调查(NDHS)的二次分析。
尼泊尔。
(1)在研究医院分娩的 75428 名妇女;(2)NDHS:12674 名年龄在 15-49 岁的妇女。
利用 2015 年 9 月至 2017 年 3 月在尼泊尔六所三级医院分娩的 75428 名妇女的数据,我们报告了这些医院出生性别比偏斜的情况,一些医院每 100 名女性出生 121 名男性。我们发现,全国代表性调查(2011NDHS)显示,男婴和女婴在医院分娩的数量没有差异。此外,我们还发现:(1)在第一个孩子是女孩的情况下,第二个孩子的出生性别比估计值明显高于我们研究中的生物学性别比;(2)多产妇女比初产妇女更有可能在产前了解胎儿的性别,并更有可能生育男孩,而且这种差异随着教育程度的提高而增加。
我们的分析支持选择性堕胎是研究医院出生性别比偏斜的主要原因。尼泊尔迫切需要全面的国家政策,不仅要计划和执行反对性别歧视堕胎的法规,还要改善尼泊尔妇女边缘化的地位,以改变这种令人震惊的男孩偏好表现。
NCT02718222。