Lamichhane Reeta, Zhao Yun, Paudel Susan, Adewuyi Emmanuel O
Department of Epidemiology and Biostatistics, School of Public Health, Curtin University, Perth, Australia.
Malteser International, Pulchowk, Laliltpur, Nepal.
BMC Public Health. 2017 Jan 10;17(1):53. doi: 10.1186/s12889-016-3922-z.
Infant mortality is one of the priority public health issues in developing countries like Nepal. The infant mortality rate (IMR) was 48 and 46 per 1000 live births for the year 2006 and 2011, respectively, a slight reduction during the 5 years' period. A comprehensive analysis that has identified and compared key factors associated with infant mortality is limited in Nepal, and, therefore, this study aims to fill the gap.
Datasets from Nepal Demographic and Health Surveys (NDHS) 2006 and 2011 were used to identify and compare the major factors associated with infant mortality. Both surveys used multistage stratified cluster sampling techniques. A total of 8707 and 10,826 households were interviewed in 2006 and 2011, with more than 99% response rate in both studies. The survival information of singleton live-born infants born 5 years preceding the two surveys were extracted from the 'childbirth' dataset. Multiple logistic regression analysis using a hierarchical modelling approach with the backward elimination method was conducted. Complex Samples Analysis was used to adjust for unequal selection probability due to the multistage stratified cluster-sampling procedure used in both NDHS.
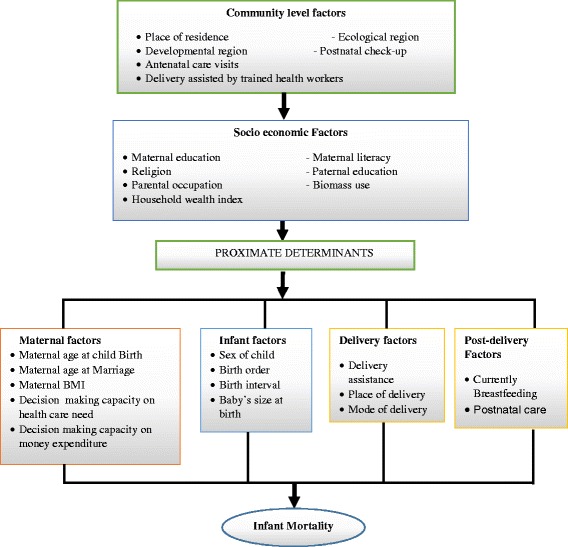
Based on NDHS 2006, ecological region, succeeding birth interval, breastfeeding status and type of delivery assistance were found to be significant predictors of infant mortality. Infants born in hilly region (AOR = 0.43, p = 0.013) and with professional assistance (AOR = 0.27, p = 0.039) had a lower risk of mortality. On the other hand, infants with succeeding birth interval less than 24 months (AOR = 6.66, p = 0.001) and those who were never breastfed (AOR = 1.62, p = 0.044) had a higher risk of mortality. Based on NDHS 2011, birth interval (preceding and succeeding) and baby's size at birth were identified to be significantly associated with infant mortality. Infants born with preceding birth interval (AOR = 1.94, p = 0.022) or succeeding birth interval (AOR = 3.22, p = 0.002) shorter than 24 months had higher odds of mortality while those born with a very large or larger than average size had significantly lowered odds (AOR = 0.17, p = 0.008) of mortality.
IMR and associated risk factors differ between NDHS 2006 and 2011 except 'succeeding birth interval' which attained significant status in the both study periods. This study identified the ecological region, birth interval, delivery assistant type, baby's birth size and breastfeeding status as significant predictors of infant mortality.
在尼泊尔等发展中国家,婴儿死亡率是重点公共卫生问题之一。2006年和2011年的婴儿死亡率分别为每1000例活产48例和46例,在这5年期间略有下降。在尼泊尔,一项全面分析已识别并比较与婴儿死亡率相关的关键因素的研究较为有限,因此,本研究旨在填补这一空白。
使用2006年和2011年尼泊尔人口与健康调查(NDHS)的数据集来识别并比较与婴儿死亡率相关的主要因素。两项调查均采用多阶段分层整群抽样技术。2006年和2011年分别共访谈了8707户和10826户家庭,两项研究的回应率均超过99%。从“分娩”数据集中提取在两次调查前5年内出生的单胎活产婴儿的生存信息。采用分层建模方法和向后剔除法进行多因素逻辑回归分析。由于NDHS采用了多阶段分层整群抽样程序,因此使用复杂样本分析来调整不等的选择概率。
基于2006年的NDHS,发现生态区域、随后的生育间隔、母乳喂养状况和分娩协助类型是婴儿死亡率的重要预测因素。出生在山区的婴儿(比值比[AOR]=0.43,p=0.013)和获得专业协助的婴儿(AOR=0.27,p=0.039)死亡风险较低。另一方面,随后生育间隔小于24个月的婴儿(AOR=6.66,p=0.001)和从未母乳喂养的婴儿(AOR=1.62,p=0.044)死亡风险较高。基于2011年的NDHS,生育间隔(之前和之后)和出生时婴儿的大小被确定与婴儿死亡率显著相关。之前生育间隔(AOR=1.94,p=0.022)或随后生育间隔(AOR=3.22,p=0.002)短于24个月的婴儿死亡几率较高,而出生时体型非常大或大于平均水平的婴儿死亡几率显著降低(AOR=0.17,p=0.008)。
2006年和2011年的NDHS中,除了“随后生育间隔”在两个研究期间均具有显著地位外,婴儿死亡率及相关风险因素有所不同。本研究确定生态区域、生育间隔、分娩协助类型、婴儿出生大小和母乳喂养状况是婴儿死亡率的重要预测因素。