Department of Abdominal Surgery, University of Helsinki and HUS Helsinki University Hospital, Haartmaninkatu 4, 00029 HUS, Helsinki, Finland.
Department of Transplantation and Liver Surgery, University of Helsinki and HUS Helsinki University Hospital, Helsinki, Finland.
Surg Endosc. 2019 Nov;33(11):3725-3731. doi: 10.1007/s00464-019-06666-5. Epub 2019 Feb 1.
While 3D laparoscopy increases surgical performance under laboratory conditions, it is unclear whether it improves outcomes in real clinical scenarios. The aim of this trial was to determine whether the 3D laparoscopy can enhance surgical efficacy in laparoscopic cholecystectomy (LCC).
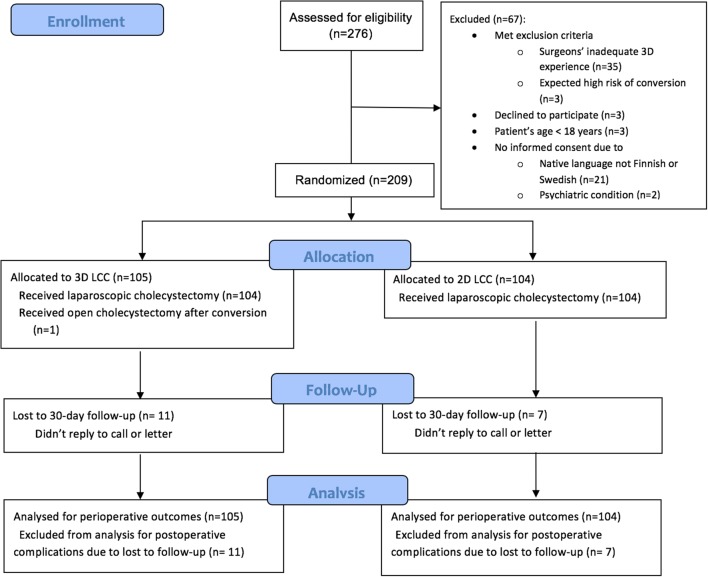
This prospective randomized controlled study was conducted between February 2015 and April 2017 in a day case unit of an academic teaching hospital. Patients scheduled for elective LCC were assessed for eligibility. The exclusion criteria were: (1) planned secondary operation in addition to LCC, (2) predicted to be high-risk for conversion, and (3) surgeons with less than five previous 3D laparoscopic procedures. Patients were operated on by 12 residents and 3 attendings. The primary endpoint was operation time. All surgeons were tested for stereoaquity (Randot® stereotest). The study was registered in ClinicalTrials.gov (NCT02357589).
A total of 210 patients were randomized; 105 to 3D laparoscopy and 104 to 2D laparoscopy. Median operation time as similar in the 3D and 2D laparoscopy groups (49 min vs. 48 min, p = 0.703). Operation times were similar in subgroup analyses for surgeon's sex (male vs. female), surgeon's status (resident vs. attending), surgeon's stereovision (stereopsis 10 vs. less than 10), surgeon's experience (performed 200 LCCs or below versus over 200 LCCs), or patient's BMI (≤ 25 vs. 25-30 vs. > 30). No differences in intra- or postoperative complications were noted between the 3D and 2D groups.
3D laparoscopy did not show any advantages over 2D laparoscopy in LCC.
虽然 3D 腹腔镜技术在实验室条件下提高了手术效果,但在真实临床环境下其是否能改善手术结局尚不清楚。本试验旨在明确 3D 腹腔镜技术是否能提高腹腔镜胆囊切除术(LC)的手术效果。
这是一项在一家学术教学医院日间病房进行的前瞻性随机对照研究,于 2015 年 2 月至 2017 年 4 月期间开展。将所有拟行择期 LC 的患者纳入研究并评估其是否符合纳入标准。排除标准包括:(1)LC 之外还计划进行其他辅助手术;(2)预计中转开腹风险较高;(3)术者 3D 腹腔镜手术经验不足 5 例。研究共纳入 12 名住院医师和 3 名主治医生,由他们分别为患者实施 3D 腹腔镜或 2D 腹腔镜手术。主要研究终点为手术时间。所有术者均进行了立体视锐度(Randot®立体测试)检测。本研究已在 ClinicalTrials.gov 注册(NCT02357589)。
共有 210 例患者被随机分配至 3D 腹腔镜组(105 例)或 2D 腹腔镜组(104 例)。3D 腹腔镜组与 2D 腹腔镜组的中位手术时间无显著差异(49 分钟比 48 分钟,p=0.703)。进一步对术者性别(男 vs. 女)、术者职称(住院医师 vs. 主治医生)、术者立体视锐度(立体视锐度 10 分及以上 vs. 小于 10 分)、术者手术经验(LC 手术经验<200 例 vs. 200 例及以上)和患者 BMI(≤25kg/m2 vs. 25-30kg/m2 vs. >30kg/m2)等亚组患者的手术时间进行分析,也均未发现 3D 腹腔镜组具有优势。两组患者的术中及术后并发症发生率无显著差异。
3D 腹腔镜技术在 LC 中并未优于 2D 腹腔镜技术。