Centre for Research in Evidence-Based Practice, Bond University, Gold Coast, Queensland, Australia.
Sydney Medical School, The University of Sydney, Sydney, New South Wales, Australia.
Health Expect. 2019 Jun;22(3):475-484. doi: 10.1111/hex.12871. Epub 2019 Feb 3.
Case-finding for dementia is practised by general practitioners (GPs) in Australia but without an awareness of community preferences. We explored the values and preferences of informed community members around case-finding for dementia in Australian general practice.
DESIGN, SETTING AND PARTICIPANTS: A before and after, mixed-methods study in Gold Coast, Australia, with ten community members aged 50-70.
A 2-day citizen/community jury. Participants were informed by experts about dementia, the potential harms and benefits of case-finding, and ethical considerations.
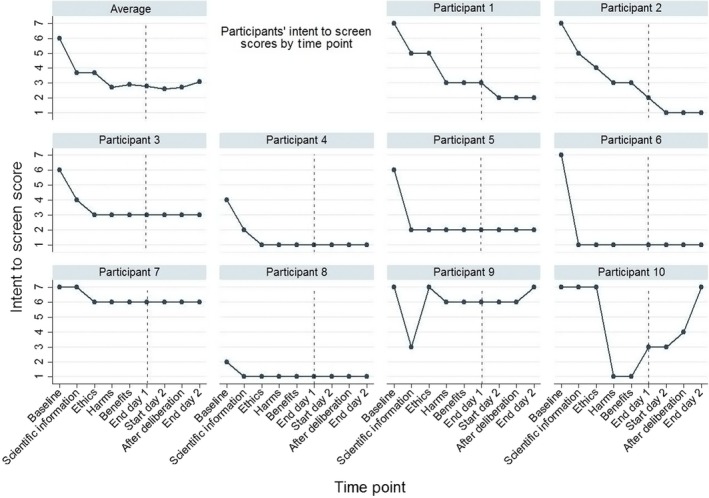
We asked participants, "Should the health system encourage GPs to practice 'case-finding' of dementia in people older than 50?" Case-finding was defined as a GP initiating testing for dementia when the patient is unaware of symptoms. We also assessed changes in participant comprehension/knowledge, attitudes towards dementia and participants' own intentions to undergo case-finding for dementia if it were suggested.
Participants voted unanimously against case-finding for dementia, citing a lack of effective treatments, potential for harm to patients and potential financial incentives. However, they recognized that case-finding was currently practised by Australian GPs and recommended specific changes to the guidelines. Participants increased their comprehension/knowledge of dementia, their attitude towards case-finding became less positive, and their intentions to be tested themselves decreased.
Once informed, community jury participants did not agree case-finding for dementia should be conducted by GPs. Yet their personal intentions to accept case-finding varied. If case-finding for dementia is recommended in the guidelines, then shared decision making is essential.
在澳大利亚,全科医生(GP)会进行痴呆症病例发现,但他们并不了解社区的偏好。我们探讨了澳大利亚全科实践中痴呆症病例发现的知情社区成员的价值观和偏好。
设计、地点和参与者:这是一项在澳大利亚黄金海岸进行的前后混合方法研究,参与者为 10 名年龄在 50-70 岁之间的社区成员。
为期两天的公民/社区陪审团。参与者由专家告知有关痴呆症的信息,包括病例发现的潜在危害和益处,以及伦理考虑因素。
我们问参与者,“卫生系统是否应该鼓励全科医生对 50 岁以上的人进行痴呆症‘病例发现’?”病例发现被定义为当患者不知道自己有症状时,全科医生开始对痴呆症进行测试。我们还评估了参与者的理解/知识、对痴呆症的态度以及他们自己如果建议进行痴呆症病例发现的意愿的变化。
参与者一致投票反对痴呆症病例发现,理由是缺乏有效的治疗方法、可能对患者造成伤害以及可能的财务激励。然而,他们认识到澳大利亚的全科医生目前正在进行病例发现,并建议对指南进行具体修改。参与者增加了对痴呆症的理解/知识,对病例发现的态度变得不那么积极,自己接受测试的意愿也降低了。
一旦知情,社区陪审团成员不同意由全科医生进行痴呆症病例发现。然而,他们自己接受病例发现的意愿存在差异。如果指南建议进行痴呆症病例发现,则需要进行共同决策。