Centro de Estudios para la Medición de la Actividad Física "CEMA". Escuela de Medicina y Ciencias de la Salud, Universidad del Rosario, Bogotá, DC, Colombia.
Grupo GICAEDS. Programa de Cultura Física, Deporte y Recreación, Universidad Santo Tomás, Bogotá, DC, Colombia.
Lipids Health Dis. 2019 Feb 4;18(1):42. doi: 10.1186/s12944-019-0981-z.
Strong evidence shows that physical inactivity increases the risk of many adverse health conditions, including major non-communicable diseases, such as cardiovascular disease (CVD), metabolic syndrome, and breast and colon cancers, and shortens life expectancy. We aimed to determine the effects of moderate (MCT)- versus high-intensity interval training (HIT) on vascular function parameters in physically inactive adults. We hypothesized that individualized HIT prescription would improve the vascular function parameters more than the MCT in a greater proportion of individuals.
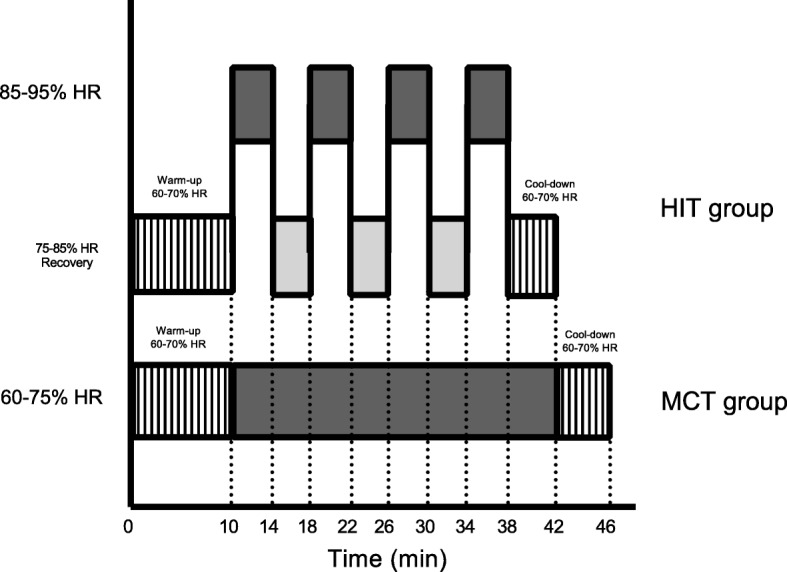
Twenty-one inactive adults were randomly allocated to receive either MCT group (60-75% of their heart rate reserve, [HRR] or HIT group (4 min at 85-95% of peak HRR), 3 days a week for 12 weeks. Vascular function (brachial artery flow-mediated dilation, FMD [%], normalized brachial artery flow-mediated dilation, FMDn [%], aortic pulse wave velocity, PWV [m·s], AIx, augmentation index: aortic and brachial [%]), were measured at baseline and over 12 weeks of training. In order for a participant to be considered a responder to improvements in vascular function parameters (FMDn and PWV), the typical error was calculated in a favorable direction.
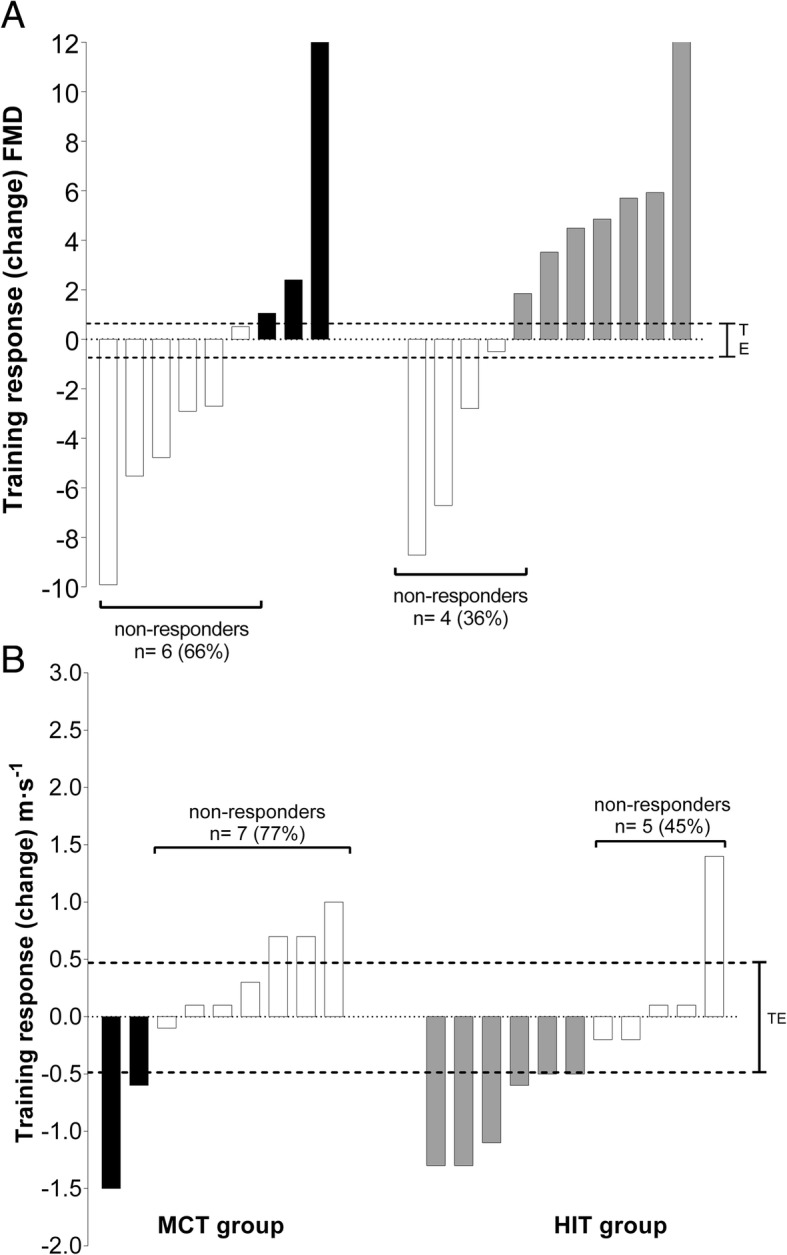
FMD changed by - 1.0% (SE 2.1, d = 0.388) in the MCT group, and + 1.8% (SE 1.8, d = 0.699) in the HIT group (no significant difference between groups: 2.9% [95% CI, - 3.0 to 8.8]. PWV changed by + 0.1 m·s (SE 0.2, d = 0.087) in the MCT group but decreased by - 0.4 m·s in the HIT group (SE 0.2, d = 0.497), with significant difference between groups: - 0.4 [95% CI, - 0.2 to - 0.7]. There was not a significant difference in the prevalence of no-responder for FMD (%) between the MCT and HIT groups (66% versus 36%, P = 0.157). Regarding PWV (m·s), an analysis showed that the prevalence of no-responder was 77% (7 cases) in the MCT group and 45% (5 cases) in the HIT group (P = 0.114).
Under the conditions of the present study, both groups experienced changed in vascular function parameters. Compared to MCT group, HIT is more efficacious for improving FMD and decreasing PWV, in physically inactive adults.
ClinicalTrials.gov NCT02738385 registered on 23 March 2016.
大量证据表明,缺乏身体活动会增加多种不良健康状况的风险,包括主要的非传染性疾病,如心血管疾病(CVD)、代谢综合征以及乳腺癌和结肠癌,并缩短预期寿命。我们旨在确定在身体不活跃的成年人中,中等强度(MCT)与高强度间歇训练(HIT)对血管功能参数的影响。我们假设,在更大比例的个体中,个体化的 HIT 处方将比 MCT 更能改善血管功能参数。
21 名不活跃的成年人被随机分配到 MCT 组(心率储备的 60-75%[HRR])或 HIT 组(4 分钟内达到峰值 HRR 的 85-95%),每周 3 天,持续 12 周。血管功能(肱动脉血流介导的扩张,FMD[%],归一化肱动脉血流介导的扩张,FMDn[%],主动脉脉搏波速度,PWV[m·s],AIx,主动脉和肱动脉的增强指数:[%])在基线和 12 周的训练中进行测量。为了确定参与者是否对血管功能参数(FMDn 和 PWV)的改善有反应,计算了有利方向的典型误差。
MCT 组的 FMD 变化为-1.0%(SE 2.1,d=0.388),HIT 组的 FMD 变化为+1.8%(SE 1.8,d=0.699)(两组间无显著差异:2.9%[95%CI,-3.0 至 8.8])。MCT 组的 PWV 增加了 0.1 m·s(SE 0.2,d=0.087),而 HIT 组的 PWV 下降了 0.4 m·s(SE 0.2,d=0.497),两组间有显著差异:-0.4 [95%CI,-0.2 至 -0.7]。MCT 和 HIT 组之间 FMD(%)的无反应者比例没有显著差异(66%与 36%,P=0.157)。关于 PWV(m·s),分析表明,MCT 组无反应者的比例为 77%(7 例),HIT 组为 45%(5 例)(P=0.114)。
在本研究的条件下,两组的血管功能参数均发生了变化。与 MCT 组相比,HIT 更能有效改善 FMD 和降低 PWV,在身体不活跃的成年人中。
ClinicalTrials.gov NCT02738385 于 2016 年 3 月 23 日注册。