Department of Integrative Physiology, University of Colorado Boulder, Boulder, Colorado, United States.
J Appl Physiol (1985). 2024 Jul 1;137(1):194-222. doi: 10.1152/japplphysiol.00188.2024. Epub 2024 May 30.
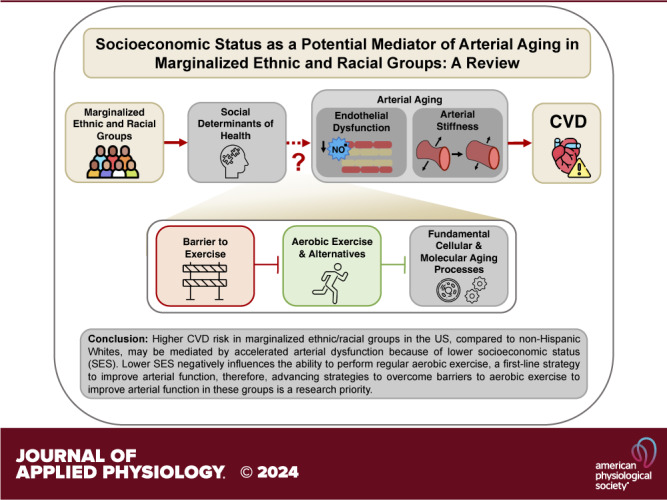
Cardiovascular diseases (CVDs) are the leading cause of death in the United States. However, disparities in CVD-related morbidity and mortality exist as marginalized racial and ethnic groups are generally at higher risk for CVDs (Black Americans, Indigenous People, South and Southeast Asians, Native Hawaiians, and Pacific Islanders) and/or development of traditional CVD risk factors (groups above plus Hispanics/Latinos) relative to non-Hispanic Whites (NHW). In this comprehensive review, we outline emerging evidence suggesting these groups experience accelerated arterial dysfunction, including vascular endothelial dysfunction and large elastic artery stiffening, a nontraditional CVD risk factor that may predict risk of CVDs in these groups with advancing age. Adverse exposures to social determinants of health (SDOH), specifically lower socioeconomic status (SES), are exacerbated in most of these groups (except South Asians-higher SES) and may be a potential mediator of accelerated arterial aging. SES negatively influences the ability of marginalized racial and ethnic groups to meet aerobic exercise guidelines, the first-line strategy to improve arterial function, due to increased barriers, such as time and financial constraints, lack of motivation, facility access, and health education, to performing conventional aerobic exercise. Thus, identifying alternative interventions to conventional aerobic exercise that ) overcome these common barriers and ) target the biological mechanisms of aging to improve arterial function may be an effective, alternative method to aerobic exercise to ameliorate accelerated arterial aging and reduce CVD risk. Importantly, dedicated efforts are needed to assess these strategies in randomized-controlled clinical trials in these marginalized racial and ethnic groups.
心血管疾病(CVDs)是美国的主要死因。然而,心血管疾病相关发病率和死亡率存在差异,因为边缘化的种族和族裔群体通常面临更高的心血管疾病风险(非裔美国人、原住民、南亚和东南亚人、夏威夷原住民和太平洋岛民)和/或发展传统心血管疾病风险因素(上述群体加上西班牙裔/拉丁裔)相对于非西班牙裔白人(NHW)。在这篇综合综述中,我们概述了一些新出现的证据,这些证据表明这些群体经历了加速的动脉功能障碍,包括血管内皮功能障碍和大弹性动脉僵硬,这是一种非传统的心血管疾病风险因素,可能预示着这些群体随着年龄的增长患心血管疾病的风险。社会决定健康因素(SDOH)的不利暴露,特别是较低的社会经济地位(SES),在这些群体中大部分(南亚裔除外- SES 较高)加剧了,可能是加速动脉老化的潜在中介因素。SES 对边缘化的种族和族裔群体满足有氧运动指南的能力产生负面影响,有氧运动指南是改善动脉功能的一线策略,因为存在增加的障碍,如时间和财务限制、缺乏动力、设施准入和健康教育,从而影响他们进行常规有氧运动的能力。因此,确定替代常规有氧运动的干预措施,这些措施)克服这些常见障碍和)针对衰老的生物学机制来改善动脉功能,可能是一种改善加速动脉老化和降低心血管疾病风险的有效替代有氧运动的方法。重要的是,需要在这些边缘化的种族和族裔群体中进行随机对照临床试验来评估这些策略。