Rohilla Seema, Garg Harender K, Singh Ishwar, Yadav Rohtas K, Dhaulakhandi Dhara B
Department of Radiodiagnosis & Imaging, Post Graduate Institute of Medical Sciences, Sharma University of Health Sciences, Rohtak, Haryana, India.
Department of Neurosurgery, Post Graduate Institute of Medical Sciences, Sharma University of Health Sciences, Rohtak, Haryana, India.
Basic Clin Neurosci. 2018 Nov-Dec;9(6):417-428. doi: 10.32598/bcn.9.6.417. Epub 2018 Nov 1.
This study was conducted to grade meningiomas based on relative Cerebral Blood Volume (rCBV) and Apparent Diffusion Coefficient (ADC) to help surgeons plan the approach and extent of operation as well as decide on the need of any adjuvant radio/chemo therapy. The current and evolving genomic, proteomic, and spectroscopic technologies are also discussed which can supplement the current radiologic methods and procedures in grading meningiomas.
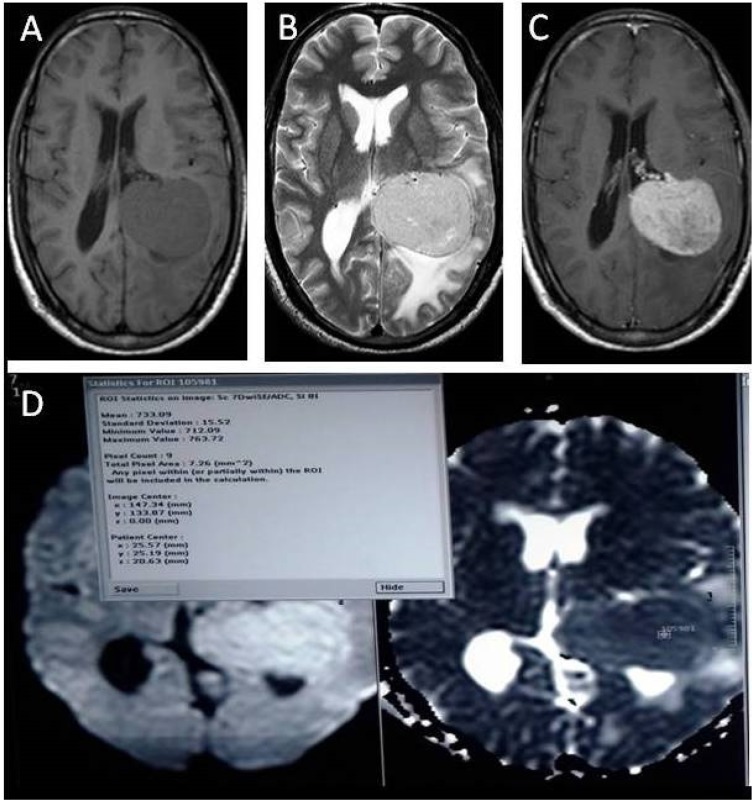
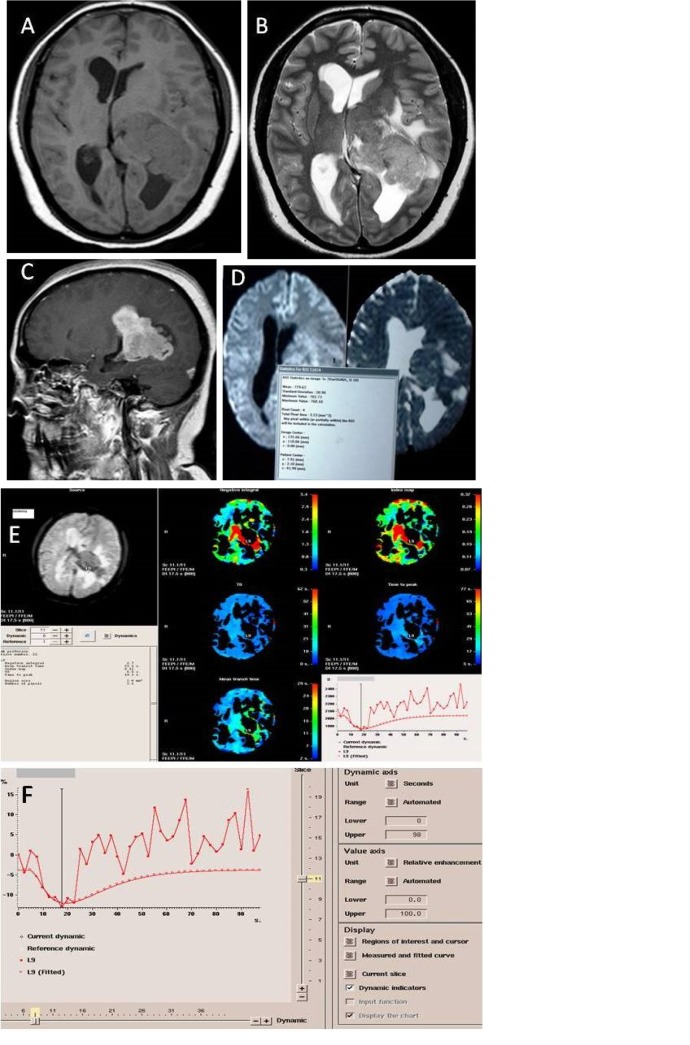
A total of 35 patients with meningioma prospectively underwent basic MR sequences (T1W, T2W, T2W/FLAIR) in axial, sagittal and coronal planes followed by Diffusion Weighted (DW) imaging having b value of 1000 (minimum ADC values used for analysis). Then, gadobenate dimeglumine/meglumine gadoterate was administered (0.1 mmol/kg at a rate of 4 mL/s) followed by saline flush (20 mL at a rate of 4 mL/s). Next, T*W/FFE dynamic images were acquired; dynamics showing maximum fall in intensity was used for creating rCBV and relative Cerebral Blood Flow (rCBF) maps and calculating rCBV.
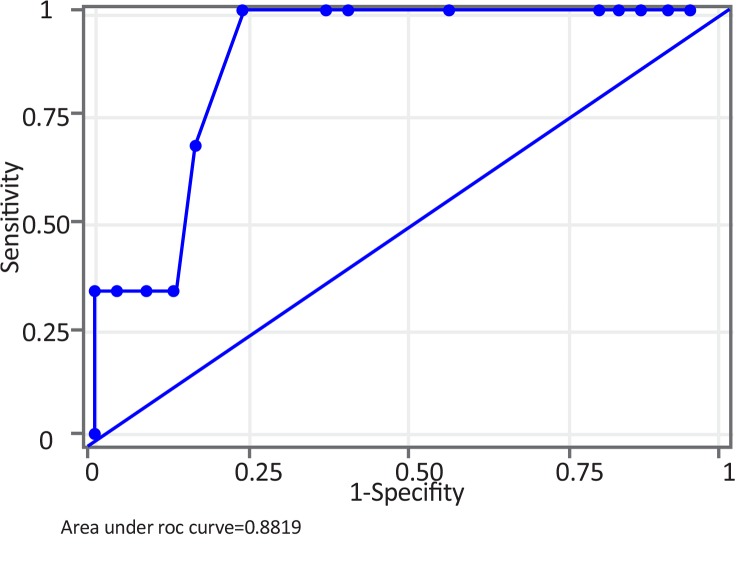
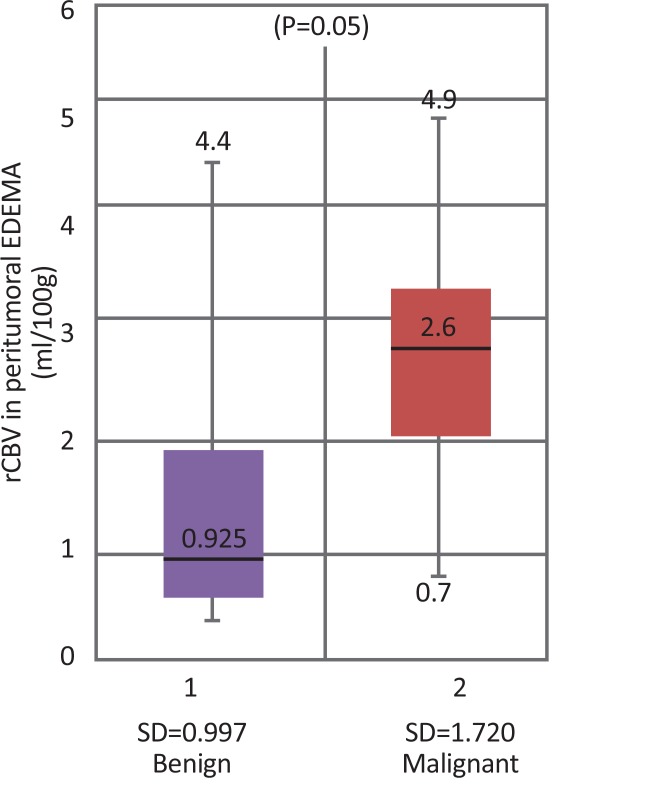
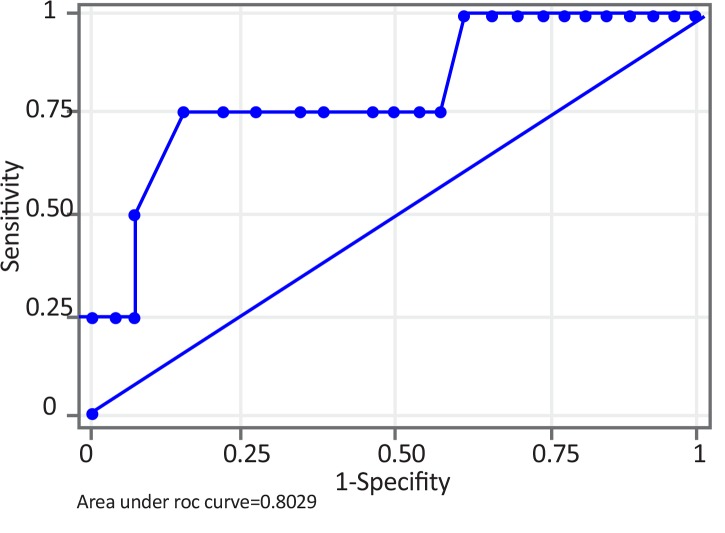
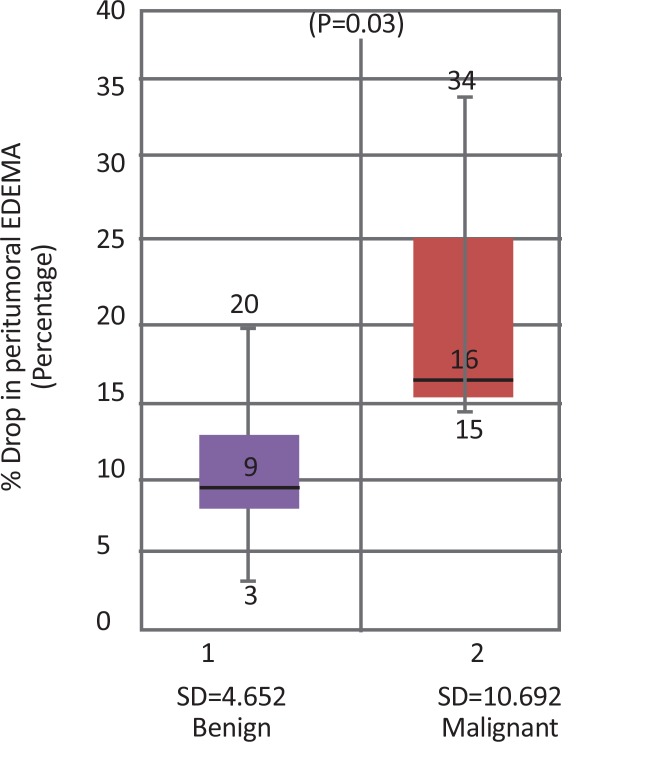
Both maximum rCBV and minimum ADC within the tumor were not significant for differentiating benign from malignant meningiomas. A cut-off maximum rCBV of 2.5 mL/100 g in peritumoral edema was 75% sensitive, 84.6% specific, and 83.3% accurate in differentiating benign from malignant meningiomas.
Benign and malignant meningiomas can be differentiated based on maximum rCBV in peritumoral edema but ADC values within the tumor are insignificant in differentiating benign and malignant tumors. rCBV values within tumor, however, may be helpful in subtyping meningiomas, especially transitional and meningothelial meningiomas.
本研究旨在根据相对脑血容量(rCBV)和表观扩散系数(ADC)对脑膜瘤进行分级,以帮助外科医生规划手术入路和范围,并决定是否需要任何辅助放疗/化疗。还讨论了当前和不断发展的基因组学、蛋白质组学和光谱技术,这些技术可以补充当前在脑膜瘤分级中的放射学方法和程序。
总共35例脑膜瘤患者前瞻性地接受了轴位、矢状位和冠状位的基本MR序列(T1W、T2W、T2W/FLAIR),随后进行b值为1000的扩散加权(DW)成像(分析时使用最小ADC值)。然后,给予钆贝葡胺/钆喷酸葡胺(0.1 mmol/kg,速率为4 mL/s),随后进行生理盐水冲洗(20 mL,速率为4 mL/s)。接下来,采集T*W/FFE动态图像;使用强度下降最大的动态图像创建rCBV和相对脑血流量(rCBF)图并计算rCBV。
肿瘤内的最大rCBV和最小ADC对于区分良性和恶性脑膜瘤均无显著意义。瘤周水肿中最大rCBV的截断值为2.5 mL/100 g,在区分良性和恶性脑膜瘤时,敏感性为75%,特异性为84.6%,准确性为83.3%。
良性和恶性脑膜瘤可根据瘤周水肿中的最大rCBV进行区分,但肿瘤内的ADC值在区分良性和恶性肿瘤方面无显著意义。然而,肿瘤内的rCBV值可能有助于脑膜瘤的亚型分类,尤其是过渡型和脑膜内皮型脑膜瘤。