Department of Colorectal Surgery, Western General Hospital, Edinburgh, UK.
Department of Anaesthesia, Western General Hospital, Edinburgh, UK.
Tech Coloproctol. 2019 Jan;23(1):15-24. doi: 10.1007/s10151-019-1927-1. Epub 2019 Feb 5.
Return of normal gastrointestinal (GI) function is a critical determinant of recovery after colorectal surgery. The aim of this meta-analysis was to evaluate whether perioperative intravenous (IV) lidocaine benefits return of gastrointestinal function after colorectal resection.
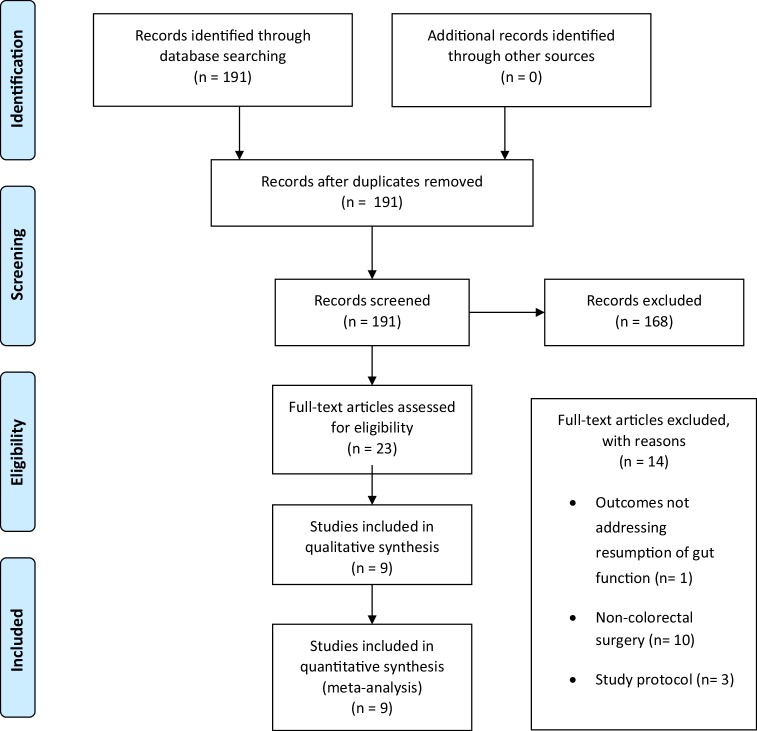
A comprehensive search of Ovid Medline, PubMed, Embase, Cochrane library, and clinicaltrials.org was performed on 1st July 2018. A manual search of reference lists was also performed. Inclusion criteria were as follows: randomized controlled trials (RCTs) of intravenous (IV) lidocaine administered perioperatively compared to placebo (0.9% saline infusion) as part of a multimodal perioperative analgesic regimen, human adults (> 16 years), and open or laparoscopic colorectal resectional surgery.
non-colorectal surgery, non-placebo comparator, children, non-general anaesthetic, and pharmacokinetic studies. The primary endpoint was time to first bowel movement. Secondary endpoints were time to first passage of flatus, time to toleration of diet, nausea and vomiting, ileus, pain scores, opioid analgesia consumption, and length of stay.
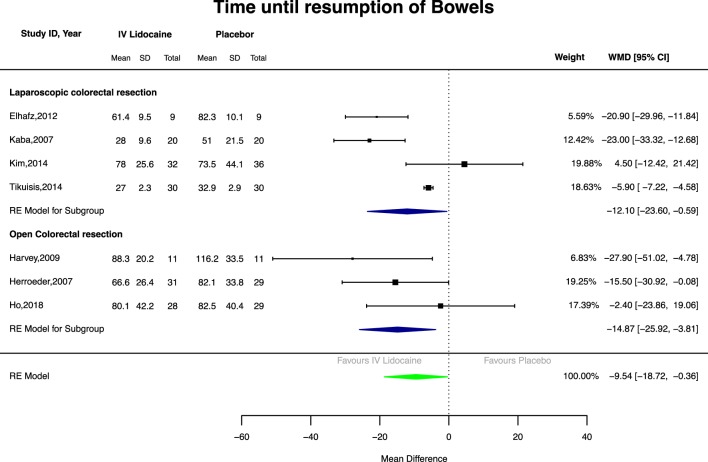
One hundred and ninety one studies were screened, with 9 RCTs meeting inclusion criteria (405 patients, four laparoscopic and five open surgery studies). IV lidocaine reduced time to first bowel movement compared to placebo [seven studies, 325 patients, mean weighted difference - 9.54 h, 95% CI 18.72-0.36, p = 0.04]. Ileus, pain scores, and length of stay were reduced with IV lidocaine compared with placebo.
Perioperative IV lidocaine may improve recovery of gastrointestinal function after colorectal surgery. Large-scale effectiveness studies to measure effect size and evaluate optimum dose/duration are warranted.
胃肠道(GI)功能的恢复是结直肠手术后康复的关键决定因素。本荟萃分析的目的是评估围手术期静脉(IV)利多卡因是否有利于结直肠切除术后胃肠道功能的恢复。
于 2018 年 7 月 1 日在 Ovid Medline、PubMed、Embase、Cochrane 图书馆和 clinicaltrials.org 进行了全面的文献检索。还手动检索了参考文献列表。纳入标准如下:静脉(IV)利多卡因与安慰剂(0.9%生理盐水输注)作为多模式围手术期镇痛方案的一部分,在人类成年人(>16 岁)中进行的比较,开腹或腹腔镜结直肠切除术。
非结直肠手术、非安慰剂对照、儿童、非全身麻醉和药代动力学研究。主要终点是首次排便时间。次要终点是首次排气时间、耐受饮食时间、恶心和呕吐、肠梗阻、疼痛评分、阿片类药物镇痛消耗和住院时间。
筛选出 191 项研究,其中 9 项 RCT 符合纳入标准(405 例患者,4 项腹腔镜手术和 5 项开腹手术研究)。与安慰剂相比,IV 利多卡因可减少首次排便时间[7 项研究,325 例患者,平均加权差异-9.54 小时,95%CI18.72-0.36,p=0.04]。与安慰剂相比,IV 利多卡因可减少肠梗阻、疼痛评分和住院时间。
围手术期 IV 利多卡因可能改善结直肠手术后胃肠道功能的恢复。需要进行大规模的有效性研究来衡量效果大小并评估最佳剂量/持续时间。