Department of Research, Cancer Registry of Norway, Oslo, Norway.
Department of Registration, Cancer Registry of Norway, Oslo, Norway.
Int J Cancer. 2019 Nov 15;145(10):2629-2638. doi: 10.1002/ijc.32195. Epub 2019 Mar 4.
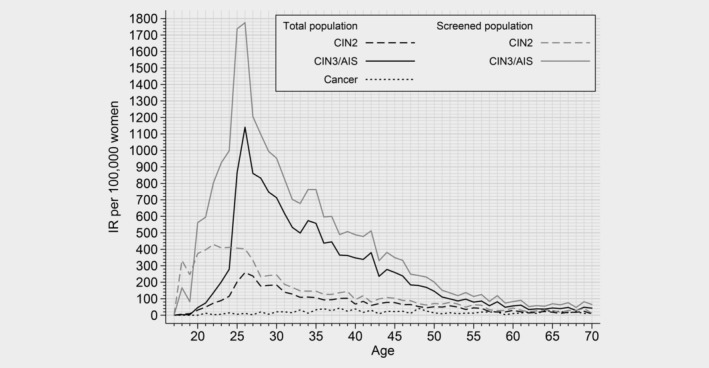
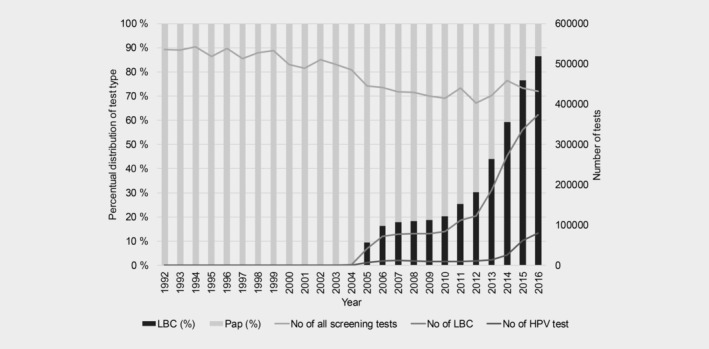
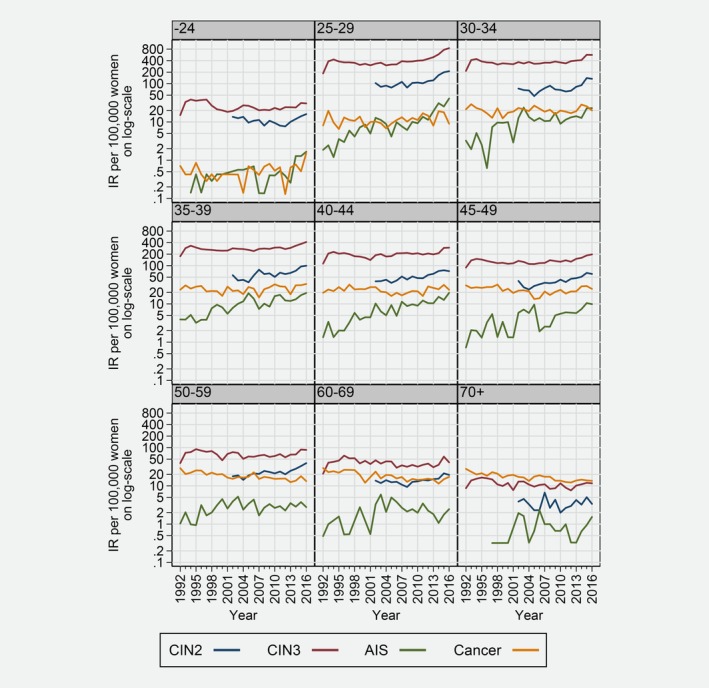
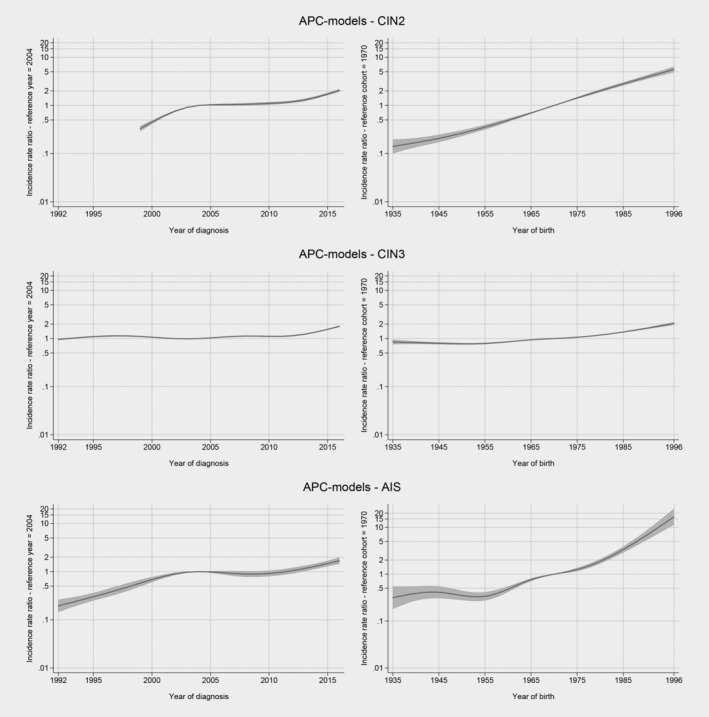
We analysed patterns in the incidence of cervical intraepithelial neoplasia grades 2 and 3 (CIN2, CIN3) and adenocarcinoma in situ (AIS) by age and histology in 1992-2016 in Norway and described changes in screening tests. Incident cases of CIN2, CIN3, AIS and cervical cancer were identified in the Cancer Registry of Norway, as were all women with at least one screening test. The annual percentage change statistic was used to assess point estimates and changes in age-specific and age-standardised incidence rates (IR). Women aged 25-29 years had the highest incidence of cervical precancerous lesions (CIN2: 192.9/10, CIN3: 737.2/10, AIS: 32.5/10 in 2016). The IR of CIN2 increased for all screening ages (25-69 years) from 3.6% to 6.7% per year. CIN3 incidence increased by 1.6% (95% confidence interval [CI] 0.6-2.6) annually. A steep increase in AIS incidence was observed in all age groups (7.1% per year, 95% CI 5.3-8.8). Changes in screening tests and the histological verification of cervical precancerous lesions alone cannot explain the steady increase in incidence we observed over the 25-year study period, and increased exposure to human papillomavirus (HPV) likely plays a role. Age-appropriate treatment of screening-detected cervical precancerous lesions is needed for effective cervical cancer control while avoiding overtreatment and related health risks. In order to perform an appropriate harm-benefit evaluation of cervical cancer control efforts, detailed information on screening technology and background risks, including HPV vaccination status, is needed to create optimal public health policy.
我们分析了 1992-2016 年在挪威,按年龄和组织学分析的宫颈上皮内瘤变 2 级和 3 级(CIN2、CIN3)和原位腺癌(AIS)的发病模式,并描述了筛查试验的变化。挪威癌症登记处确定了 CIN2、CIN3、AIS 和宫颈癌的发病病例,以及所有至少接受过一次筛查试验的妇女。使用年度百分比变化统计数据评估点估计和年龄特异性及年龄标准化发病率(IR)的变化。25-29 岁的女性宫颈癌前病变(CIN2:2016 年为 192.9/10,CIN3:737.2/10,AIS:32.5/10)发病率最高。所有筛查年龄(25-69 岁)的 CIN2IR 每年增加 3.6%至 6.7%。CIN3 发病率每年增加 1.6%(95%置信区间 [CI] 0.6-2.6)。所有年龄组的 AIS 发病率都急剧上升(每年 7.1%,95%CI 5.3-8.8)。我们观察到,在 25 年的研究期间,筛查试验的变化和宫颈癌前病变的组织学验证都不能解释发病率的持续上升,HPV(人乳头瘤病毒)的暴露增加可能发挥了作用。需要对筛查发现的宫颈癌前病变进行适当年龄的治疗,以有效控制宫颈癌,同时避免过度治疗和相关的健康风险。为了对宫颈癌控制工作进行适当的危害-效益评估,需要详细了解筛查技术和背景风险的信息,包括 HPV 疫苗接种状况,以制定最佳的公共卫生政策。