Jonklaas Jacqueline, Tefera Eshetu, Shara Nawar
Division of Endocrinology, Georgetown University, Washington, DC, United States.
Department of Biostatistics and Biomedical Informatics, Medstar Health Research Institute, Hyattsville, MD, United States.
Front Endocrinol (Lausanne). 2019 Jan 30;10:31. doi: 10.3389/fendo.2019.00031. eCollection 2019.
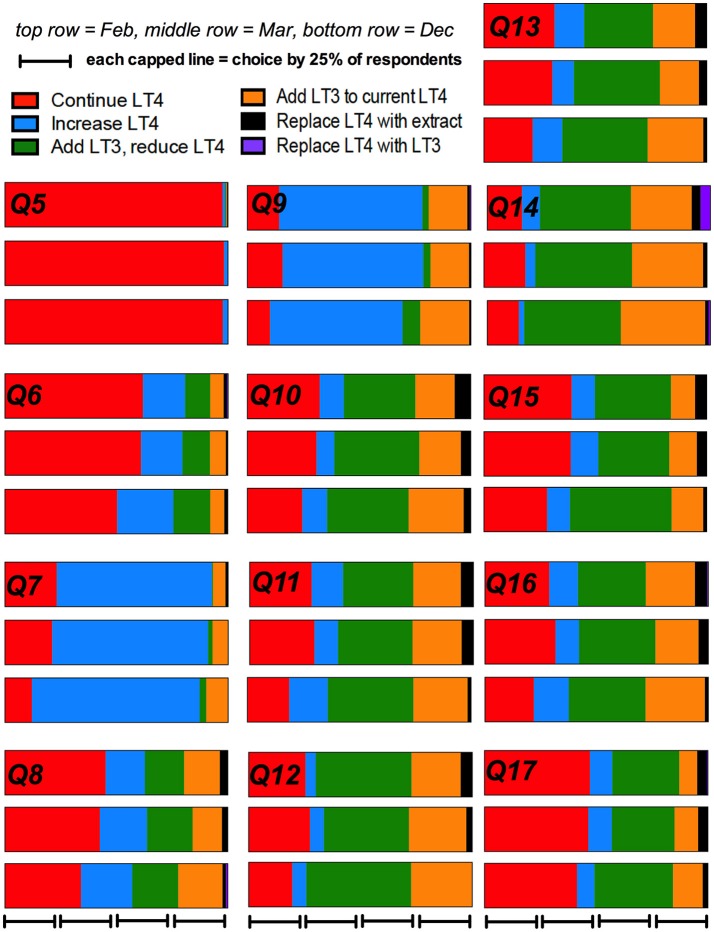
Hypothyroid patients frequently request specific therapies from their physicians. Combination therapy is vigorously discussed at professional meetings. We wished to determine if physician prescribing patterns for hypothyroidism changed during 2017 after specific educational events. A survey addressing treatment of hypothyroidism was emailed to American Thyroid Association (ATA) members on three occasions in 2017. The Spring emails were sent prior to a satellite symposium addressing hypothyroidism, and prior to the annual Endocrine Society and ATA meetings; the December emails were sent after these events. Physicians were presented with thirteen theoretical patients and chose from 6 therapeutic options, including levothyroxine, synthetic combination therapy, thyroid extract, and liothyronine monotherapy. The patient scenarios successively incorporated factors potentially providing reasons for considering combination therapy. Multivariate repeated measures logistic regression analyses first examined effects of physician characteristics on prescribing the various therapies. Then, analyses also incorporated timing, by comparing prescribing patterns in February, March, and December. In analyses of prescribing levothyroxine monotherapy vs. any T3 therapy, there was a trend of borderline significance ( = 0.053) for T3 therapy to be prescribed more in December compared with February-March combined. When multivariate analyses were performed controlling for time and physician characteristics, choice of therapy was only significantly affected by country of practice (OR 1.7, CI 1.3-2.2). Physician choice of therapies was also examined for the options of continuing (1) levothyroxine, vs. (2) increasing levothyroxine, (3) adding liothyronine either with or without levothyroxine reduction, or (4) replacing levothyroxine with desiccated thyroid extract or liothyronine. When multivariate analyses incorporating time and physician characteristics were performed, respondents in December (OR 1.5, CI 1.0-2.3) and those practicing in North America (OR 1.8, CI 1.2-2.6) were more likely to prescribe liothyronine. This survey shows that although current North American guidelines do not recommend combination therapy, such therapy is being prescribed more over time and is also more commonly prescribed in North America. It is possible our guidelines are failing to incorporate evidence that physicians are considering when prescribing combination therapy. Such evidence could include data about patient preferences, and this needs to be a focus of future studies.
甲状腺功能减退患者经常向医生寻求特定的治疗方法。联合治疗在专业会议上得到了热烈讨论。我们希望确定在2017年特定的教育活动之后,医生对甲状腺功能减退症的处方模式是否发生了变化。2017年,我们分三次向美国甲状腺协会(ATA)成员发送了一封关于甲状腺功能减退症治疗的调查问卷。春季的邮件是在一次关于甲状腺功能减退症的卫星研讨会之前、内分泌学会和ATA年度会议之前发送的;12月的邮件是在这些活动之后发送的。向医生展示了13个虚拟患者案例,并让他们从6种治疗方案中进行选择,包括左甲状腺素、合成联合治疗、甲状腺提取物和单药治疗的碘塞罗宁。患者案例依次纳入了可能为考虑联合治疗提供理由的因素。多变量重复测量逻辑回归分析首先研究了医生特征对各种治疗方案处方的影响。然后,通过比较2月、3月和12月的处方模式,分析还纳入了时间因素。在分析左甲状腺素单药治疗与任何含T3治疗方案时,与2月至3月的合并数据相比,12月开具T3治疗方案的趋势具有临界显著性(P = 0.053)。在对时间和医生特征进行控制的多变量分析中,治疗方案的选择仅受到执业国家的显著影响(比值比1.7,置信区间1.3 - 2.2)。我们还研究了医生对以下治疗方案的选择:(1)继续使用左甲状腺素,与(2)增加左甲状腺素剂量、(3)添加碘塞罗宁(无论是否减少左甲状腺素剂量),或(4)用干燥甲状腺提取物或碘塞罗宁替代左甲状腺素。在进行纳入时间和医生特征的多变量分析时,12月的受访者(比值比1.5,置信区间1.0 - 2.3)以及在北美执业的受访者(比值比1.8,置信区间1.2 - 2.6)更有可能开具碘塞罗宁。这项调查表明,尽管目前北美指南不推荐联合治疗,但随着时间的推移,这种治疗方案的处方量越来越多,并且在北美也更常被开具。有可能我们的指南未能纳入医生在开具联合治疗处方时所考虑的证据。这些证据可能包括有关患者偏好的数据,这需要成为未来研究的重点。