Princess Máxima Center for Pediatric Oncology, Utrecht, the Netherlands.
Department of Pediatric Hematology and Oncology, Erasmus MC - Sophia Children's Hospital, Rotterdam, the Netherlands.
PLoS One. 2019 Feb 14;14(2):e0210646. doi: 10.1371/journal.pone.0210646. eCollection 2019.
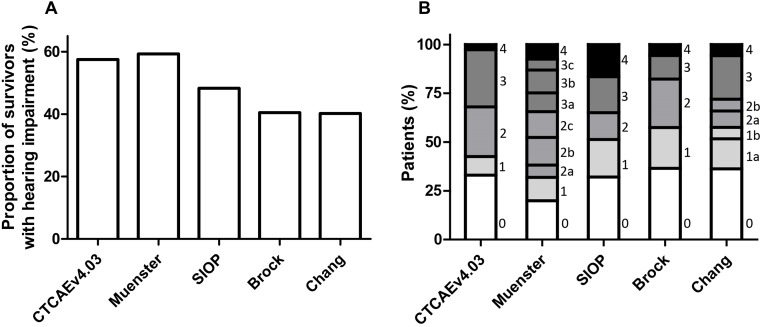
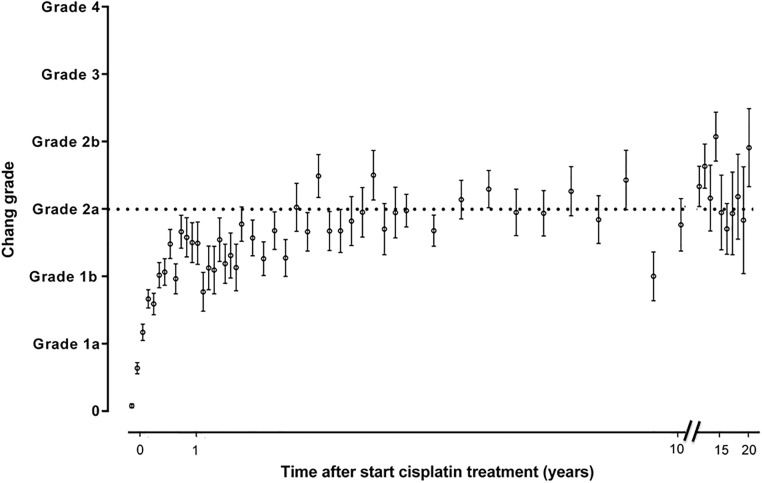
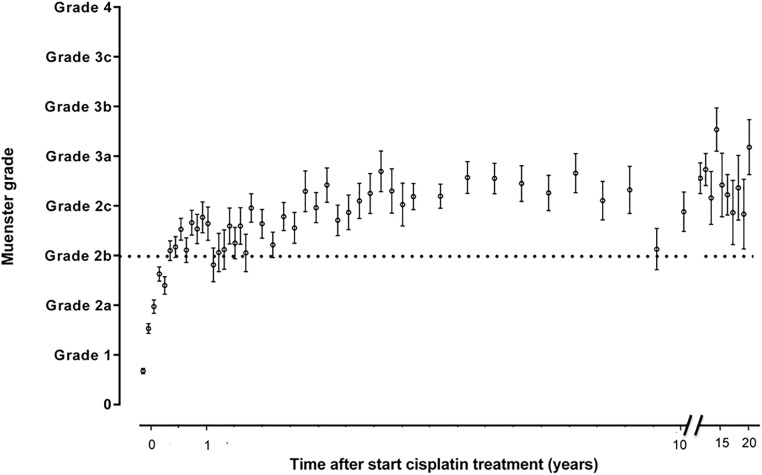
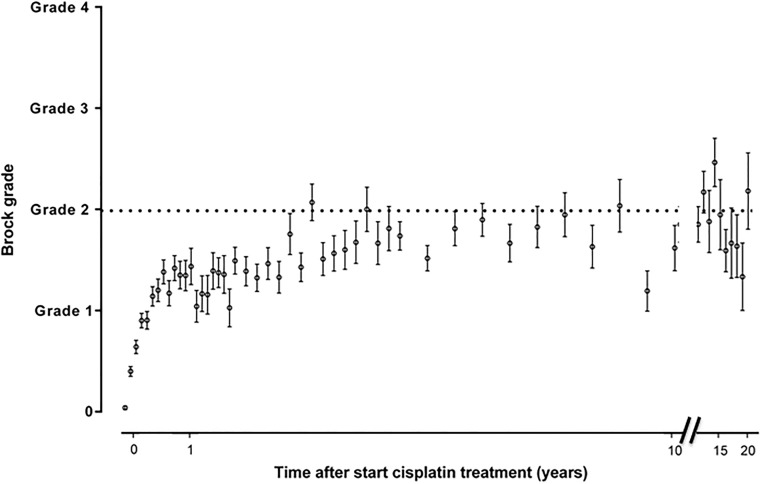
Childhood cancer patients treated with platinums often develop hearing loss and the degree is classified according to different scales globally. Our objective was to compare concordance between five well-known ototoxicity scales used for childhood cancer patients. Audiometric test results (n = 654) were evaluated longitudinally and graded according Brock, Chang, International Society of Pediatric Oncology (SIOP) Boston, Muenster scales and the U.S. National Cancer Institute Common Technology Criteria for Adverse Events (CTCAE) version 4.03. Adverse effects of grade 2, 3 and 4 are considered to reflect a degree of hearing loss sufficient to interfere with day-to-day communication (> = Chang grade 2a; > = Muenster grade 2b). We term this "deleterious hearing loss". A total number of 3,799 audiograms were evaluated. The prevalence of deleterious hearing loss according to the last available audiogram of each patient was 59.3% (388/654) according to Muenster, 48.2% (315/653) according to SIOP, 40.5% (265/652) according to Brock, 40.3% (263/652) according to Chang, and 57.5% (300/522) according to CTCAEv4.03. Overall concordance between the scales ranged from ĸ = 0.636 (Muenster vs. Chang) to ĸ = 0.975 (Brock vs. Chang). Muenster detected hearing loss the earliest in time, followed by Chang, SIOP and Brock. Generally good concordance between the scales was observed but there is still diversity in definitions of functional outcomes, such as differences in distribution levels of severity of hearing loss, and additional intermediate scales taking into account losses <40 dB as well. Regardless of the scale used, hearing function decreases over time and therefore, close monitoring of hearing function at baseline and with each cycle of platinum therapy should be conducted.
接受铂类药物治疗的儿童癌症患者常发生听力损失,且全球范围内根据不同的量表对其进行分级。我们的目标是比较用于儿童癌症患者的五种著名耳毒性量表之间的一致性。对(n = 654)例患者的纵向听力学测试结果进行评估,并根据 Brock、Chang、国际儿童肿瘤学会(SIOP)波士顿、明斯特量表和美国国家癌症研究所不良事件通用技术标准(CTCAE)第 4.03 版进行分级。2 级、3 级和 4 级的不良影响被认为反映了足以干扰日常交流的听力损失程度(> = Chang 2a 级;> = Muenster 2b 级)。我们将此称为“有害听力损失”。共评估了 3799 次听力图。根据每位患者的最后一次可用听力图,根据 Muenster 量表,59.3%(388/654)的患者发生有害听力损失,根据 SIOP 量表,48.2%(315/653)的患者发生有害听力损失,根据 Brock 量表,40.5%(265/652)的患者发生有害听力损失,根据 Chang 量表,40.3%(263/652)的患者发生有害听力损失,根据 CTCAE v4.03 量表,57.5%(300/522)的患者发生有害听力损失。这些量表之间的整体一致性范围为 k = 0.636(Muenster 与 Chang)至 k = 0.975(Brock 与 Chang)。Muenster 最早发现听力损失,其次是 Chang、SIOP 和 Brock。尽管这些量表之间具有良好的一致性,但在功能结果的定义方面仍存在多样性,例如听力损失严重程度的分布水平存在差异,以及考虑到听力损失<40dB 的额外中间量表。无论使用哪种量表,听力功能都会随时间下降,因此,应在基线和铂类药物治疗的每个周期密切监测听力功能。