RTI International, 701 13th ST NW, Suite 750, Washington, DC, USA.
Epidemiology Department, UNC Gillings School of Global Public Health, 2103 McGavran-Greenberg Hall, CB #7435, Chapel Hill, NC, 27599, USA.
BMC Med. 2019 Feb 15;17(1):25. doi: 10.1186/s12916-019-1256-2.
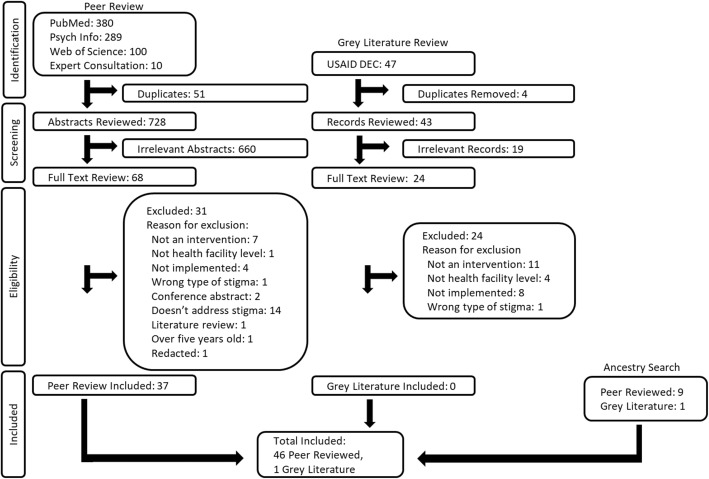
Stigma in health facilities undermines diagnosis, treatment, and successful health outcomes. Addressing stigma is fundamental to delivering quality healthcare and achieving optimal health. This correspondence article seeks to assess how developments over the past 5 years have contributed to the state of programmatic knowledge-both approaches and methods-regarding interventions to reduce stigma in health facilities, and explores the potential to concurrently address multiple health condition stigmas. It is supported by findings from a systematic review of published articles indexed in PubMed, Psychinfo and Web of Science, and in the United States Agency for International Development's Development Experience Clearinghouse, which was conducted in February 2018 and restricted to the past 5 years. Forty-two studies met inclusion criteria and provided insight on interventions to reduce HIV, mental illness, or substance abuse stigma. Multiple common approaches to address stigma in health facilities emerged, which were implemented in a variety of ways. The literature search identified key gaps including a dearth of stigma reduction interventions in health facilities that focus on tuberculosis, diabetes, leprosy, or cancer; target multiple cadres of staff or multiple ecological levels; leverage interactive technology; or address stigma experienced by health workers. Preliminary results from ongoing innovative responses to these gaps are also described.The current evidence base of stigma reduction in health facilities provides a solid foundation to develop and implement interventions. However, gaps exist and merit further work. Future investment in health facility stigma reduction should prioritize the involvement of clients living with the stigmatized condition or behavior and health workers living with stigmatized conditions and should address both individual and structural level stigma.
卫生机构中的污名化现象会破坏诊断、治疗和健康结果。解决污名问题是提供优质医疗保健和实现最佳健康的基础。这篇通讯文章旨在评估过去 5 年来的发展情况如何为卫生机构中减少污名化干预措施的方案知识(包括方法和方法)做出贡献,并探讨同时解决多种健康状况污名的潜力。它得到了 2018 年 2 月进行的、针对过去 5 年发表在 PubMed、Psychinfo 和 Web of Science 以及美国国际开发署发展经验信息中心的已发表文章的系统评价的支持。42 项研究符合纳入标准,为减少 HIV、精神疾病或药物滥用污名的干预措施提供了见解。在卫生机构中解决污名问题的多个常见方法已经出现,并以各种方式实施。文献检索确定了关键差距,包括缺乏针对结核病、糖尿病、麻风病或癌症的卫生机构减少污名化干预措施;针对多个员工群体或多个生态层次;利用互动技术;或解决卫生工作者经历的污名。还描述了正在对这些差距做出创新性应对的初步结果。目前,卫生机构减少污名的证据基础为制定和实施干预措施提供了坚实的基础。然而,仍然存在差距,值得进一步研究。未来在卫生机构减少污名方面的投资应优先考虑涉及受污名化状况或行为影响的患者和患有污名化状况的卫生工作者,并应解决个人和结构性污名问题。