White Ruth, Hayes Chris, Boyes Allison W, Chiu Simon, Paul Christine L
Hunter Integrated Pain Service, Hunter New England Health, Newcastle, NSW, Australia,
School of Medicine and Public Health, University of Newcastle, NSW, Australia,
J Pain Res. 2019 Jan 22;12:467-475. doi: 10.2147/JPR.S168785. eCollection 2019.
General practitioners' (GPs) views about deprescribing prescription opioid analgesics (POAs) may influence the care provided for patients experiencing chronic noncancer pain (CNCP). There are limited data addressing GPs' beliefs about deprescribing, including their decisions to deprescribe different types of POAs.
To determine the proportion of GPs who hold attitudes congruent with local pain stewardship, describe their deprescribing decisions, and determine whether type of POA influences deprescribing.
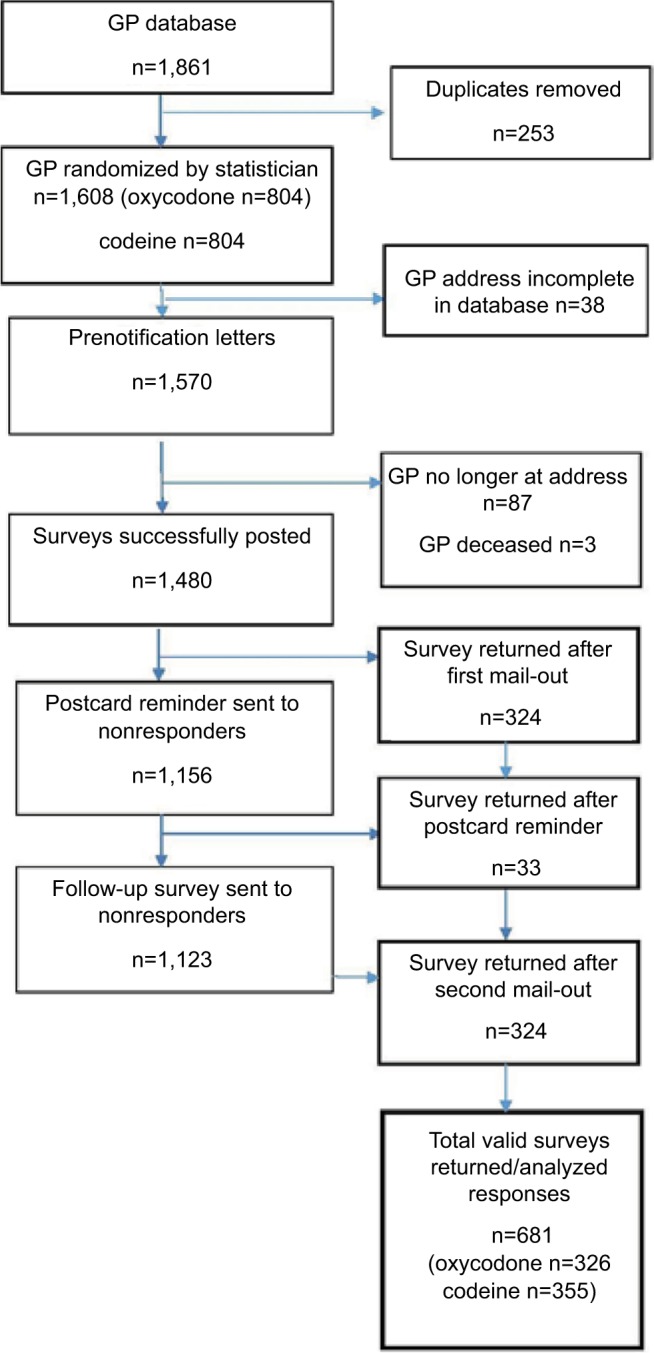
In 2016, a cross-sectional survey of all GPs (n=1,570) in one mixed urban and regional primary health network (PHN) in Australia was undertaken.
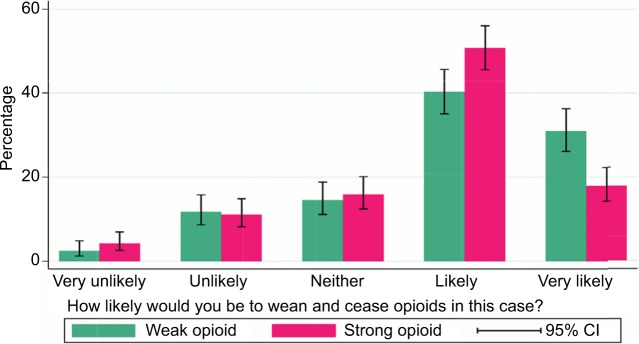
A mailed self-report questionnaire assessed agreement with local guidelines for treating CNCP; influences on deprescribing POAs and likelihood of deprescribing in a hypothetical case involving either oral codeine or oxycodone.
A response rate of 46% was achieved. Approximately half (54%) of GPs agreed POAs should be reserved for people with acute, cancer pain or palliative care and a third (32%) did not agree that a medication focus has limited benefits for peoples' long-term quality of life and function. Most (77%) GPs were less likely to deprescribe when effective alternate treatments were lacking, while various patient factors (eg, fear of weaning) were reported to decrease the likelihood of deprescribing for 25% of GPs. A significantly higher proportion of GPs reported being very likely to deprescribe codeine compared to the equivalent opioid dose of oxycodone for a hypothetical patient.
Many GPs in the PHN hold attitudes at odds with local guidance that opioids are a nonsuperior treatment for CNCP. Attitudinal barriers to deprescribing include: a lack of consistent approach to deprescribing opioids as a class of drugs, perceived lack of effective treatment alternatives and patient fear of deprescribing. Therefore, the next step in this target population is to appropriately train and support GPs in how to apply the evidence in practice and how to support patients appropriately.
全科医生(GP)对停用处方阿片类镇痛药(POA)的看法可能会影响为慢性非癌性疼痛(CNCP)患者提供的护理。关于全科医生对停药的看法,包括他们停用不同类型POA的决定的数据有限。
确定持有与当地疼痛管理态度一致的全科医生比例,描述他们的停药决定,并确定POA类型是否会影响停药。
2016年,对澳大利亚一个城乡混合的初级卫生保健网络(PHN)中的所有全科医生(n = 1570)进行了横断面调查。
通过邮寄自填问卷评估对治疗CNCP当地指南的认同度;对停用POA的影响以及在涉及口服可待因或羟考酮的假设案例中停用的可能性。
回复率为46%。大约一半(54%)的全科医生同意POA应仅用于急性、癌性疼痛或姑息治疗患者,三分之一(32%)的全科医生不同意以药物为重点对人们的长期生活质量和功能益处有限。大多数(77%)全科医生在缺乏有效的替代治疗时不太可能停药,而各种患者因素(如害怕减量)据报告使25%的全科医生停药的可能性降低。与假设患者使用等效阿片剂量的羟考酮相比,报告称非常可能停用可待因的全科医生比例显著更高。
PHN中的许多全科医生持有的态度与当地关于阿片类药物并非治疗CNCP的优势疗法的指导意见不一致。停药的态度障碍包括:作为一类药物,缺乏一致的停用阿片类药物的方法,认为缺乏有效的替代治疗以及患者对停药的恐惧。因此,针对这一目标人群的下一步是对全科医生进行适当培训并提供支持,使其了解如何在实践中应用证据以及如何适当地支持患者。