Akbaba Sati, Lang Kristin, Held Thomas, Herfarth Klaus, Rieber Juliane, Plinkert Peter, Auffarth Gerd U, Rieken Stefan, Debus Juergen, Adeberg Sebastian
Department of Radiation Oncology, University Hospital Heidelberg, Heidelberg 69120, Germany,
Heidelberg Institute of Radiation Oncology (HIRO), National Center for Radiation Research in Oncology (NCRO), University Hospital Heidelberg, Heidelberg 69120, Germany,
Cancer Manag Res. 2019 Feb 1;11:1155-1166. doi: 10.2147/CMAR.S190051. eCollection 2019.
We evaluated treatment outcomes of CIRT in an active raster-scanning technique alone or in combination with IMRT for lacrimal gland tumors.
A total of 24 patients who received CIRT for a malignant lacrimal gland tumor at the HIT between 2009 and 2018 were analyzed retrospectively for LC, OS, and distant progression-free survival (DPFS) using Kaplan-Meier estimates. Toxicity was assessed according to the CTCAE version 5.
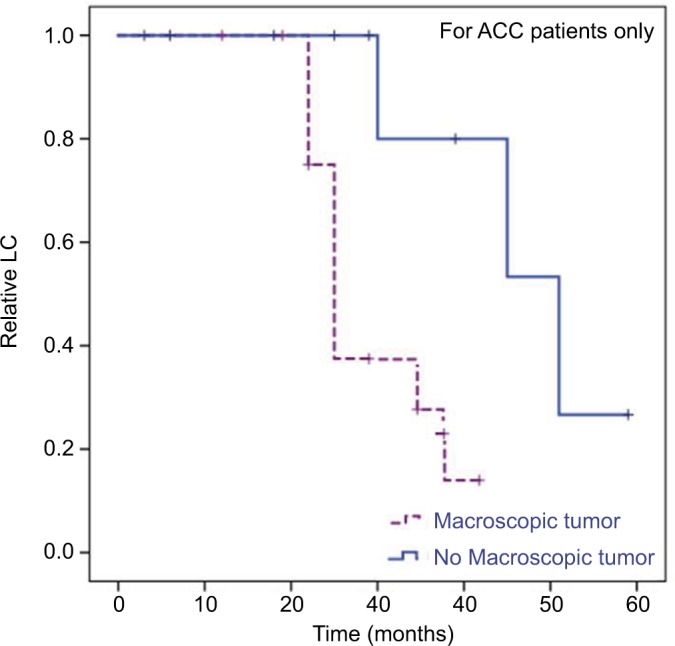
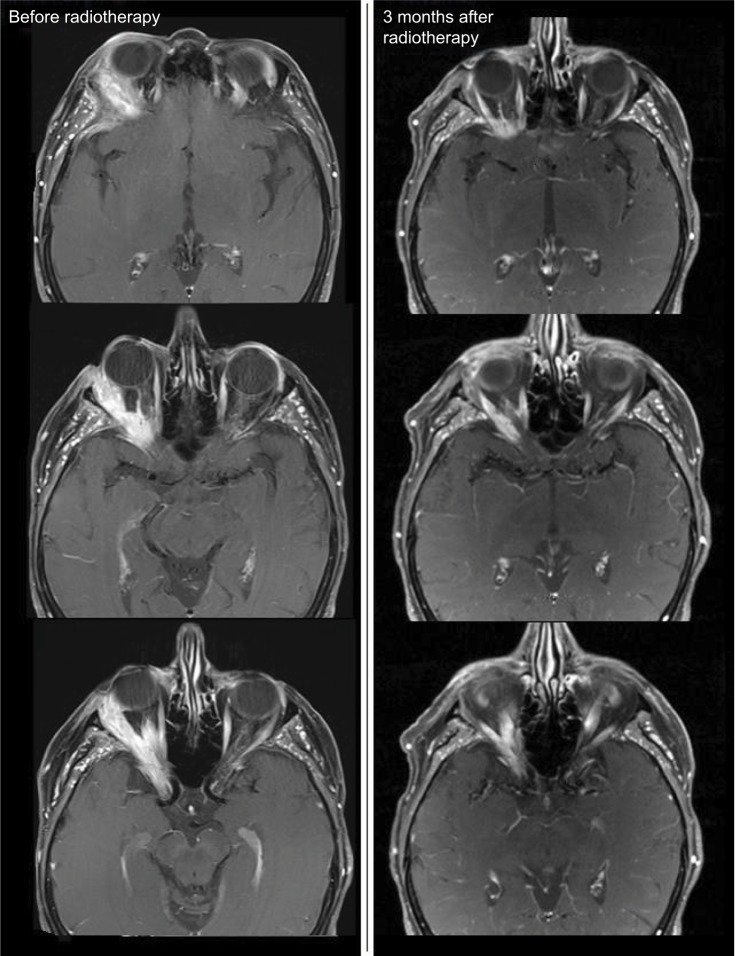
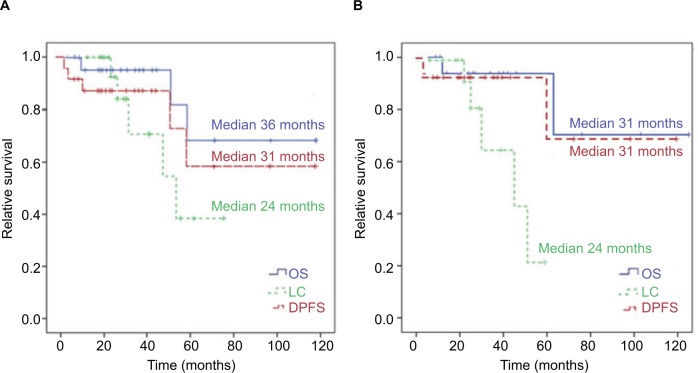
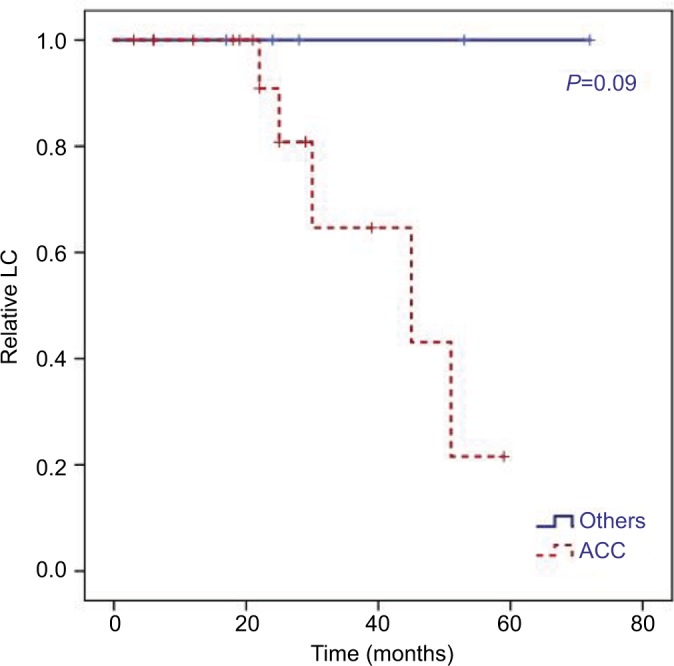
Median follow-up was 30 months and overall median LC, OS, and DPFS 24 months, 36 months, and 31 months, respectively. Two-year LC, OS, and DPFS of 93%, 96%, and 87% with CIRT was achieved for all patients. Local failure occurred only in patients with ACC and after a median follow-up of 30 months after the completion of RT (n=5, 21%; =0.09). We identified a significant negative impact of a macroscopic tumor disease, which was diagnosed on planning CT or MRI before RT, on LC (=0.026). In contrast, perineural spread (=0.661), T stage (=0.552), and resection margins in operated patients (=0.069) had no significant impact on LC. No grade ≥3 acute or grade >3 chronic toxicity occurred. Late grade 3 side effects were identified in form of a wound-healing disorder 3 months after RT in one patient and temporal lobe necrosis 6 months after RT in another (n=2, 8%).
Accelerated hypofractionated active raster-scanning CIRT for relative radio-resistant malignant lacrimal gland tumors results in adequate LC rates and moderate acute and late toxicity. Nevertheless, LC for ACC histology remains challenging and risk factors for local recurrence are still unclear. Further follow-up is necessary to evaluate long-term clinical outcome.
我们评估了单纯采用主动光栅扫描技术的碳离子放疗(CIRT)或联合调强放疗(IMRT)治疗泪腺肿瘤的疗效。
回顾性分析2009年至2018年期间在海德堡离子束治疗中心(HIT)接受CIRT治疗恶性泪腺肿瘤的24例患者的局部控制(LC)、总生存期(OS)和远处无进展生存期(DPFS),采用Kaplan-Meier法进行估计。根据美国国立癌症研究所不良事件通用术语标准第5版(CTCAE v5)评估毒性。
中位随访时间为30个月,总体中位LC、OS和DPFS分别为24个月、36个月和31个月。所有患者采用CIRT治疗的2年LC、OS和DPFS分别达到93%、96%和87%。局部失败仅发生在腺样囊性癌(ACC)患者中,放疗结束后中位随访30个月时出现(n = 5,21%;P = 0.09)。我们发现放疗前在计划CT或MRI上诊断的宏观肿瘤病变对LC有显著负面影响(P = 0.026)。相比之下,神经周围扩散(P = 0.661)、T分期(P = 0.552)和手术患者的切缘(P = 0.069)对LC无显著影响。未发生≥3级急性毒性或>3级慢性毒性。1例患者在放疗后3个月出现伤口愈合障碍,另1例在放疗后6个月出现颞叶坏死,为晚期3级副作用(n = 2,8%)。
对于相对放射抗拒的恶性泪腺肿瘤,采用加速分割主动光栅扫描CIRT可获得足够的LC率,且急性和晚期毒性适中。然而,ACC组织学类型的LC仍然具有挑战性,局部复发的危险因素仍不清楚。需要进一步随访以评估长期临床结果。