Department of Epidemiology and Biostatistics, College of Health Sciences, School of Public Health, Makerere University, P.O.BOX, 7072, Kampala, Uganda.
Department of Disease Control and Environmental Health, College of Health Sciences, School of Public Health, Makerere University, Kampala, Uganda.
Malar J. 2019 Feb 21;18(1):44. doi: 10.1186/s12936-019-2681-6.
Indoor residual spraying (IRS) with Actellic 300 CS was conducted in Lira District between July and August 2016. No formal assessment has been conducted to estimate the effect of spraying with Actellic 300 CS on malaria morbidity in the Ugandan settings. This study assessed malaria morbidity trends before and after IRS with Actellic 300 CS in Lira District in Northern Uganda.
The study employed a mixed methods design. Malaria morbidity records from four health facilities were reviewed, focusing on 6 months before and after the IRS intervention. The outcome of interest was malaria morbidity defined as; proportion of outpatient attendance due to total malaria, proportion of outpatient attendance due to confirmed malaria and proportion of malaria case numbers confirmed by microscopy or rapid diagnostic test. Since malaria morbidity was based on count data, an ordinary Poisson regression model was used to obtain percentage point change (pp) in monthly malaria cases before and after IRS. A household survey was also conducted in 159 households to determine IRS coverage and factors associated with spraying. A modified Poisson regression model was fitted to determine factors associated with household spray status.
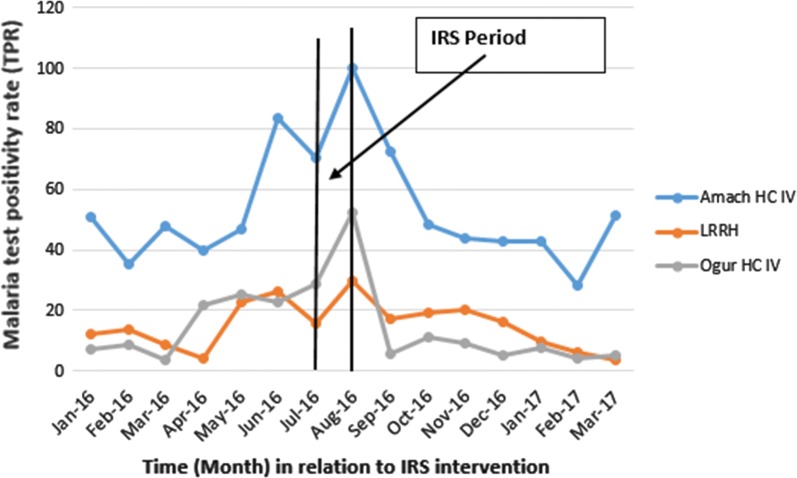
The proportion of outpatient attendance due to malaria dropped from 18.7% before spraying to 15.1% after IRS. The proportion of outpatient attendance due to confirmed malaria also dropped from 5.1% before spraying to 4.0% after the IRS intervention. There was a decreasing trend in malaria test positivity rate (TPR) for every unit increase in month after spraying. The decreasing trend in TPR was more prominent 5-6 months after the IRS intervention (Adj. pp = - 0.60, P-value = 0.015; Adj. pp = - 1.19, P-value < 0.001). The IRS coverage was estimated at 89.3%. Households of respondents who were formally employed or owned any form of business were more likely to be unsprayed; (APR = 5.81, CI 2.72-12.68); (APR = 3.84, CI 1.20-12.31), respectively.
Coverage of IRS with Actellic 300 CS was high and was associated with a significant decline in malaria related morbidity 6 months after spraying.
2016 年 7 月至 8 月,在利拉区进行了使用 Actellic 300 CS 的室内滞留喷洒。尚未进行正式评估来估计在乌干达环境中使用 Actellic 300 CS 喷洒对疟疾发病率的影响。本研究评估了在北乌干达利拉区进行使用 Actellic 300 CS 的室内滞留喷洒前后疟疾发病率的趋势。
该研究采用混合方法设计。对四个卫生机构的疟疾发病率记录进行了审查,重点是喷洒干预前和干预后 6 个月。感兴趣的结果是疟疾发病率,定义为:因总疟疾而就诊的门诊就诊比例、因确诊疟疾而就诊的门诊就诊比例和经显微镜检查或快速诊断测试确诊的疟疾病例数比例。由于疟疾发病率是基于计数数据,因此使用普通泊松回归模型来获得喷洒前后每月疟疾病例的百分比变化(pp)。还在 159 户家庭中进行了一项家庭调查,以确定室内滞留喷洒覆盖率以及与喷洒相关的因素。拟合修正泊松回归模型以确定与家庭喷洒状况相关的因素。
喷洒前因疟疾而就诊的门诊就诊比例从 18.7%下降到喷洒后的 15.1%。喷洒前因确诊疟疾而就诊的门诊就诊比例也从 5.1%下降到喷洒后的 4.0%。随着喷洒后月份的增加,疟疾检测阳性率(TPR)呈下降趋势。在喷洒后 5-6 个月,TPR 的下降趋势更为明显(调整后的 pp=-0.60,P 值=0.015;调整后的 pp=-1.19,P 值<0.001)。室内滞留喷洒覆盖率估计为 89.3%。正式受雇或拥有任何形式企业的受访者的家庭更有可能未喷洒;(调整后的优势比(APR)=5.81,CI 2.72-12.68);(调整后的优势比(APR)=3.84,CI 1.20-12.31)。
使用 Actellic 300 CS 进行室内滞留喷洒的覆盖率很高,与喷洒后 6 个月疟疾相关发病率的显著下降有关。