Sandal Shaifali, Charlebois Kathleen, Fiore Julio F, Wright David Kenneth, Fortin Marie-Chantal, Feldman Liane S, Alam Ahsan, Weber Catherine
Division of Nephrology, Department of Medicine, McGill University Health Centre, Montreal, QC, Canada.
Research Institute of the McGill University Health Centre, Montreal, QC, Canada.
Can J Kidney Health Dis. 2019 Feb 13;6:2054358119828389. doi: 10.1177/2054358119828389. eCollection 2019.
Living donor kidney transplantation (LDKT) has several advantages over deceased donor kidney transplantation. Yet rates of living donation are declining in Canada and there exists significant interprovincial variability. Efforts to improve living donation tend to focus on the patient and barriers identified at their level, such as not knowing how to ask for a kidney or lack of education. These efforts favor those who have the means and the support to find living donors. Thus, a Canadian Institutes of Health Research (CIHR)-organized workshop recommended that education efforts to understand and remove barriers should focus on health professionals (HPs). Despite this, little attention has been paid to what they identify as barriers to discussing LDKT with their patients.
Our aim was to explore HP-identified barriers to discuss living donation with patients in 3 provinces of Canada with low (Quebec), moderate (Ontario), and high (British Columbia) rates of LDKT.
This study consists of an interpretive descriptive approach as it enables to move beyond description and inform clinical practice.
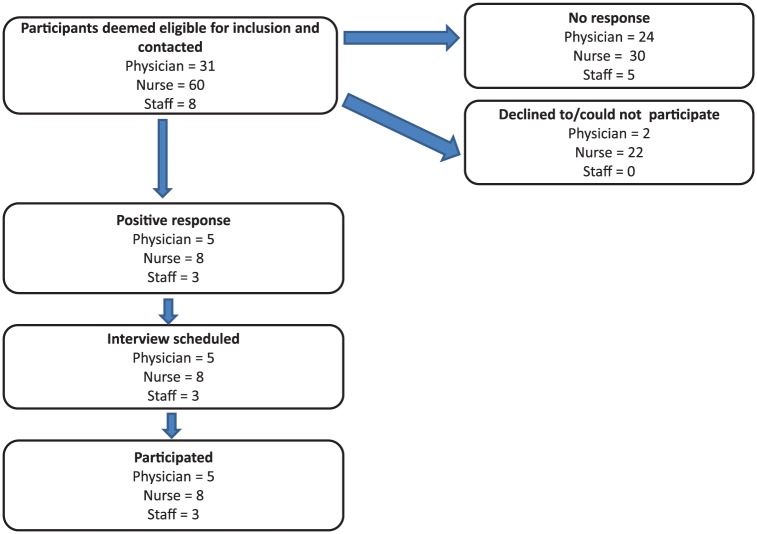
Purposive criterion and quota sampling were used to recruit HPs from Quebec, Ontario, and British Columbia who are involved in the care of patients with kidney disease and/or with transplant coordination.
Not applicable.
Semistructured interviews were conducted. The interview guide was developed based on a preliminary analytical framework and a review of the literature.
Thematic analysis was used to analyze the data stemming from the interviews. The coding process comprised of a deductive and inductive approach, and the use of a qualitative analysis software (NVivo 11). Following this, themes were identified and developed. Interviews were conducted until thematic saturation was obtained. In total, we conducted 16 telephone interviews as thematic saturation was attained.
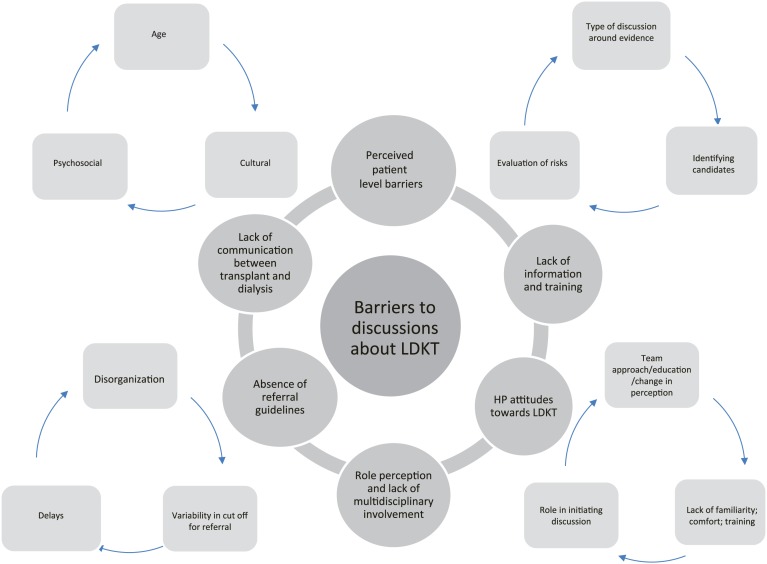
Six predominant themes emerged: (1) lack of communication between transplant and dialysis teams, (2) absence of referral guidelines, (3) role perception and lack of multidisciplinary involvement, (4) HP's lack of information and training, (5) negative attitudes of some HP toward LDKT, (6) patient-level barriers as defined by the HP. HPs did mention patients' attitudes and some characteristics as the main barriers to discussions about living donation; this was noted in all provinces. HPs from Ontario and British Columbia indicated multiple strategies being implemented to address some of these barriers. Those from Ontario mentioned strategies that center on the core principles of provincial-level standardization, while those from British Columbia center on engaging the entire multidisciplinary team and improved role perception. We noted a dearth of such efforts in Quebec; however, efforts around education and promotion, while tentative, have emerged.
Social desirability and selection bias. Our analysis might not be applicable to other provinces.
HPs involved with the referral and coordination of transplantation play a major role in access to LDKT. We have identified challenges they face when discussing living donation with their patients that warrant further assessment and research to inform policy change.
活体供肾移植(LDKT)相对于尸体供肾移植具有若干优势。然而,加拿大的活体捐赠率正在下降,且省际间存在显著差异。改善活体捐赠的努力往往侧重于患者以及在患者层面所发现的障碍,比如不知道如何请求他人捐赠肾脏或缺乏相关教育。这些努力有利于那些有能力和支持来寻找活体供者的人。因此,加拿大卫生研究院(CIHR)组织的一次研讨会建议,旨在理解和消除障碍的教育努力应聚焦于卫生专业人员(HP)。尽管如此,对于他们所认定的在与患者讨论LDKT时存在的障碍,却很少有人关注。
我们的目的是探讨在加拿大活体供肾移植率低(魁北克)、中等(安大略)和高(不列颠哥伦比亚)的3个省份中,卫生专业人员所认定的在与患者讨论活体捐赠时存在的障碍。
本研究采用解释性描述方法,因为它能够超越描述层面并为临床实践提供信息。
采用目的抽样标准和配额抽样方法,从魁北克、安大略和不列颠哥伦比亚招募参与肾病患者护理和/或移植协调工作的卫生专业人员。
不适用。
进行半结构化访谈。访谈指南是基于一个初步分析框架和文献综述制定的。
采用主题分析法对访谈所得数据进行分析。编码过程包括演绎和归纳方法,并使用定性分析软件(NVivo 11)。在此之后,确定并发展主题。持续进行访谈直至达到主题饱和。总共进行了16次电话访谈,因为已达到主题饱和。
出现了六个主要主题:(1)移植团队与透析团队之间缺乏沟通,(2)缺乏转诊指南,(3)角色认知与多学科参与不足,(4)卫生专业人员缺乏信息和培训,(5)一些卫生专业人员对LDKT持消极态度,(6)卫生专业人员所定义的患者层面的障碍。卫生专业人员确实提到患者的态度和一些特征是关于活体捐赠讨论的主要障碍;所有省份均有此情况。安大略和不列颠哥伦比亚的卫生专业人员表示正在实施多种策略来应对其中一些障碍。安大略的卫生专业人员提到的策略以省级标准化的核心原则为中心,而不列颠哥伦比亚的卫生专业人员则以让整个多学科团队参与并改善角色认知为中心。我们注意到魁北克在这方面的努力较少;然而,围绕教育和推广的努力虽尚处于初步阶段,但已经出现。
社会期望性和选择偏差。我们的分析可能不适用于其他省份。
参与移植转诊和协调工作的卫生专业人员在获得活体供肾移植方面发挥着重要作用。我们已经确定了他们在与患者讨论活体捐赠时所面临的挑战,这些挑战值得进一步评估和研究,以为政策变革提供信息依据。