Department of Trauma Surgery, Technical University Munich, Hospital Rechts der Isar, Munich, Germany.
Institute for Research in Operative Medicine (IFOM), University of Witten/Herdecke, Cologne, Germany.
PLoS One. 2019 Feb 22;14(2):e0212095. doi: 10.1371/journal.pone.0212095. eCollection 2019.
The temporal distribution of trauma mortality has been classically described as a trimodal pattern with an immediate, early and late peak. In modern health care systems this time distribution has changed.
Data from the TraumaRegister DGU was analysed retrospectively. Between 2002 and 2015, all registered in-hospital deaths with an Injury Severity Score (ISS) ≥ 16 were evaluated considering time of death, trauma mechanism, injured body area, age distribution, rates of sepsis and multiple organ failure. Pre-hospital and post-discharge trauma deaths were not considered.
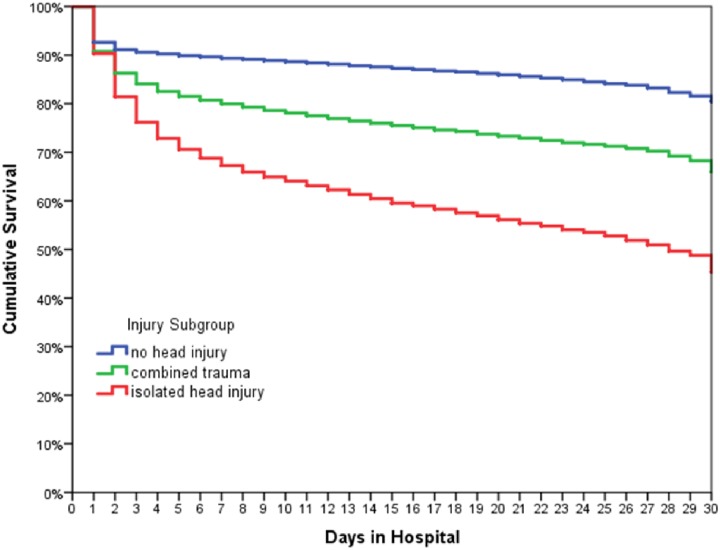
78 310 severely injured patients were registered, non-survivors constituted 14 816, representing an in-hospital mortality rate of 18.9%. Mean ISS of non-survivors was 36.0±16.0, 66.7% were male, mean age was 59.5±23.5. Within the first hour after admission to hospital, 10.8% of deaths occurred, after 6 hours the percentage increased to 25.5%, after 12 hours 40.0%, after 24 hours 53.2% and within the first 48 hours 61.9%. Mortality showed a constant temporal decrease. Severe head injury (defined by Abbreviated Injury Scale, AIS-Head≥3) was found in 76.4% of non-survivors. Patients with an isolated head injury showed a more distinct decrease in survival rate, which was accentuated in the first days after admission. The correlation of age and time of death showed a proportional increase with age (55-74a). The rate of sepsis and multiple organ failure among non-survivors was 11.5% and 70.1%, respectively.
In a modern trauma care system, the mortality distribution of severely injured patients has changed its pattern, where especially the third peak is no longer detectable.
创伤死亡率的时间分布一直被经典地描述为三峰模式,即立即、早期和晚期高峰。在现代医疗保健系统中,这种时间分布已经发生了变化。
回顾性分析创伤登记处 DGU 的数据。在 2002 年至 2015 年间,评估了所有损伤严重程度评分(ISS)≥16 且住院死亡的患者,考虑死亡时间、创伤机制、受伤身体部位、年龄分布、脓毒症和多器官衰竭的发生率。未考虑院前和出院后创伤死亡。
共登记了 78310 例严重创伤患者,非幸存者 14816 例,院内死亡率为 18.9%。非幸存者的平均 ISS 为 36.0±16.0,男性占 66.7%,平均年龄为 59.5±23.5。在入院后第一个小时内,10.8%的死亡发生,6 小时后,该比例增加到 25.5%,12 小时后增加到 40.0%,24 小时后增加到 53.2%,48 小时内增加到 61.9%。死亡率呈持续时间递减。非幸存者中严重头部损伤(定义为简明损伤评分 AIS-Head≥3)占 76.4%。孤立性头部损伤患者的生存率下降更为明显,这种下降在入院后几天内更为明显。年龄与死亡时间的相关性呈比例增加,与年龄呈正相关(55-74a)。非幸存者中脓毒症和多器官衰竭的发生率分别为 11.5%和 70.1%。
在现代创伤救治体系中,严重创伤患者的死亡率分布发生了变化,尤其是第三高峰已不再明显。