Department of Renal Medicine, Singapore General Hospital, Singapore, Singapore.
Singapore Eye Research Institute, Singapore National Eye Centre, Singapore, Singapore.
PLoS One. 2019 Feb 22;14(2):e0212590. doi: 10.1371/journal.pone.0212590. eCollection 2019.
Chronic kidney disease (CKD) contributes significant morbidity and mortality among Asians; hence interventions should focus on those most at-risk of progression. However, current end stage renal failure (ESRF) risk stratification tools are complex and not validated in multi-ethnic Asians. We hence aimed to develop an ESRF risk prediction model by taking into account ethnic differences within a fairly homogenous socioeconomic setting and using parameters readily accessible to primary care clinicians managing the vast majority of patients with CKD.
We performed a prospective cohort study of 1970 adults with CKD estimated glomerular filtration rate <60 ml/min/1.73m2 or albuminuria >30 mg/g from the population-based Singapore Epidemiology of Eye Diseases study (n = 10,033). Outcome was incident ESRF, ascertained by linkage to the Singapore Renal Registry until 2015.
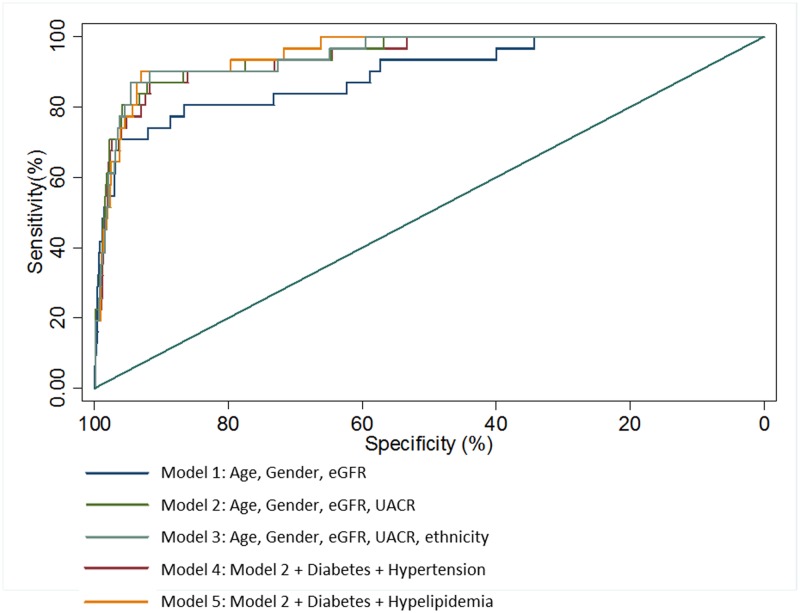
Mean follow up was 8.5 ± 1.8 years and ESRF occurred in 32 individuals (1.6%). ESRF incidence rates were 2.8, 0.8 and 2.6 per 1000 patient years in Malays, Indians and Chinese respectively. The best ESRF prediction model included age, gender, eGFR and albuminuria (calibration χ2 = 0.45, P = 0.93; C-statistic 0.933, 95% confidence interval (CI) 0.889-0.978, p = 0.01; AIC 356). Addition of ethnicity improved discrimination marginally (C statistic 0.942, 95% CI 0.903-0.981, p = 0.21). Addition of clinical variables such as diabetes and hyperlipidemia did not improve model performance significantly.
We affirmed the utility of commonly available clinical information (age, gender, eGFR and UACR) in prognosticating ESRF for multi-ethnic Asians with CKD.
慢性肾脏病(CKD)在亚洲人群中导致了大量的发病率和死亡率;因此,干预措施应侧重于那些最有可能进展的人群。然而,目前的终末期肾衰竭(ESRF)风险分层工具较为复杂,并且在多民族亚洲人群中尚未得到验证。因此,我们旨在开发一种 ESRF 风险预测模型,该模型考虑到了在相当同质的社会经济环境中存在的种族差异,并使用了初级保健临床医生管理绝大多数 CKD 患者时易于获得的参数。
我们对来自基于人群的新加坡眼病流行病学研究(n = 10,033)中的 1970 名估计肾小球滤过率<60 ml/min/1.73m2 或白蛋白尿>30 mg/g 的 CKD 成年人进行了前瞻性队列研究。结局是通过与新加坡肾脏登记处进行链接确定的,直到 2015 年。
平均随访 8.5 ± 1.8 年,共有 32 名患者(1.6%)发生 ESRF。马来人、印度人和中国人的 ESRF 发生率分别为 2.8、0.8 和 2.6/1000 患者年。最佳 ESRF 预测模型包括年龄、性别、eGFR 和白蛋白尿(校准 χ2 = 0.45,P = 0.93;C 统计量 0.933,95%置信区间(CI)0.889-0.978,p = 0.01;AIC 356)。添加种族可略微提高区分度(C 统计量 0.942,95%CI 0.903-0.981,p = 0.21)。添加临床变量(如糖尿病和高脂血症)并不能显著提高模型性能。
我们证实了常用临床信息(年龄、性别、eGFR 和 UACR)在预测多民族亚洲 CKD 患者 ESRF 方面的效用。