Lanspa Michael J, Olsen Troy D, Wilson Emily L, Leguyader Mary Louise, Hirshberg Eliotte L, Anderson Jeffrey L, Brown Samuel M, Grissom Colin K
1Critical Care Echocardiography Service, Intermountain Medical Center, 5121 S Cottonwood St, Murray, UT 84157 USA.
2Division of Pulmonary and Critical Care Medicine, University of Utah, 30 N 1900 E, 701 Wintrobe, Salt Lake City, UT 84132 USA.
J Intensive Care. 2019 Feb 20;7:14. doi: 10.1186/s40560-019-0367-3. eCollection 2019.
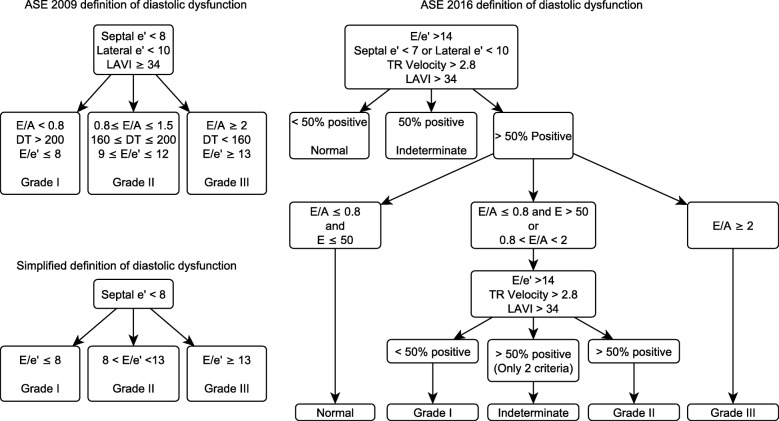
Guidelines for grading diastolic dysfunction poorly categorize septic patients. We compared how well the American Society of Echocardiography (ASE) 2009 and 2016 definitions and a simplified definition categorized septic patients.
We studied septic patients who received a transthoracic echocardiogram within 24 h of admission to an ICU. We categorized patients according to ASE 2009 and 2016 definitions and a definition using /', a surrogate for left ventricular filling pressure. We assessed 28-day all-cause mortality and the presence of pre-existing diabetes, hypertension, or myocardial infarction. We tested for associations among diastolic grade, comorbidities, and outcomes using logistic regression.
We studied 398 patients. Mortality was 23%. The simplified definition categorized more patients than ASE 2016 (78% vs. 71%, = 0.035); both definitions categorized more patients than ASE 2009 (34%, < 0.001 for both comparisons). Higher grades of diastolic dysfunction were associated with hypertension (ASE 2016, simplified), myocardial infarction (ASE 2009, simplified), and diabetes (simplified). Grade of diastolic dysfunction was not associated with mortality by any definition. Of 199 patients categorized as normal by ASE 2016, 40% had an abnormal /' > 9 and 7% had a severely abnormal /e' > 13.
The ASE 2016 definition categorizes more septic patients than the ASE 2009 definition, but it does not categorize the diastolic function of a third of septic patients. ASE 2016 designates many patients with elevated /' as normal. A simplified definition categorized patients with less ambiguity and is associated with relevant comorbidities.
舒张功能障碍分级指南对脓毒症患者的分类效果不佳。我们比较了美国超声心动图学会(ASE)2009年和2016年的定义以及一种简化定义对脓毒症患者的分类情况。
我们研究了入住重症监护病房(ICU)24小时内接受经胸超声心动图检查的脓毒症患者。我们根据ASE 2009年和2016年的定义以及使用/'(左心室充盈压的替代指标)的定义对患者进行分类。我们评估了28天全因死亡率以及是否存在既往糖尿病、高血压或心肌梗死。我们使用逻辑回归测试舒张功能分级、合并症和结局之间的关联。
我们研究了398例患者。死亡率为23%。简化定义分类的患者比ASE 2016年定义的更多(78%对71%,P = 0.035);两种定义分类的患者都比ASE 2009年定义的更多(34%,两种比较P均<0.001)。舒张功能障碍更高分级与高血压(ASE 2016年、简化定义)、心肌梗死(ASE 2009年、简化定义)和糖尿病(简化定义)相关。无论采用何种定义,舒张功能障碍分级均与死亡率无关。在ASE 2016年分类为正常的199例患者中,40%的患者/'异常>9,7%的患者/e'严重异常>13。
ASE 2016年定义分类的脓毒症患者比ASE 2009年定义的更多,但它没有对三分之一的脓毒症患者的舒张功能进行分类。ASE 2016年将许多/'升高的患者指定为正常。一种简化定义对患者的分类歧义较少,且与相关合并症有关。