Department of Health Sciences, Brock University, St Catharines, Ontario, Canada.
Department of Public Health, Erasmus MC University Medical Center, Rotterdam, the Netherlands.
JAMA Netw Open. 2019 Mar 1;2(3):e190204. doi: 10.1001/jamanetworkopen.2019.0204.
Low-dose computed tomography lung cancer screening is most effective when applied to high-risk individuals.
To develop and validate a risk prediction model that incorporates low-dose computed tomography screening results.
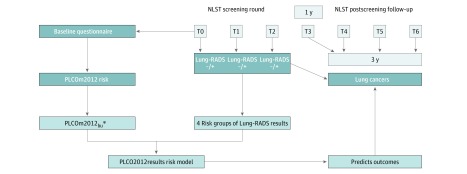
DESIGN, SETTING, AND PARTICIPANTS: A logistic regression risk model was developed in National Lung Screening Trial (NLST) Lung Screening Study (LSS) data and was validated in NLST American College of Radiology Imaging Network (ACRIN) data. The NLST was a randomized clinical trial that recruited participants between August 2002 and April 2004, with follow-up to December 31, 2009. This secondary analysis of data from the NLST took place between August 10, 2013, and November 1, 2018. Included were LSS (n = 14 576) and ACRIN (n = 7653) participants who had 3 screens, adequate follow-up, and complete predictor information.
Incident lung cancers occurring 1 to 4 years after the third screen (202 LSS and 96 ACRIN). Predictors included scores from the validated PLCOm2012 risk model and Lung CT Screening Reporting & Data System (Lung-RADS) screening results.
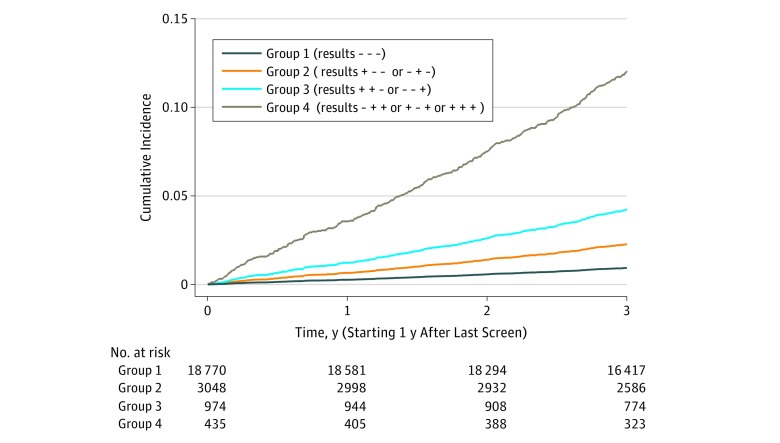
Overall, the mean (SD) age of 22 229 participants was 61.3 (5.0) years, 59.3% were male, and 90.9% were of non-Hispanic white race/ethnicity. During follow-up, 298 lung cancers were diagnosed in 22 229 individuals (1.3%). Eight result combinations were pooled into 4 groups based on similar associations. Adjusted for PLCOm2012 risks, compared with participants with 3 negative screens, participants with 1 positive screen and last negative had an odds ratio (OR) of 1.93 (95% CI, 1.34-2.76), and participants with 2 positive screens with last negative or 2 negative screens with last positive had an OR of 2.66 (95% CI, 1.60-4.43); when 2 or more screens were positive with last positive, the OR was 8.97 (95% CI, 5.76-13.97). In ACRIN validation data, the model that included PLCOm2012 scores and screening results (PLCO2012results) demonstrated significantly greater discrimination (area under the curve, 0.761; 95% CI, 0.716-0.799) than when screening results were excluded (PLCOm2012) (area under the curve, 0.687; 95% CI, 0.645-0.728) (P < .001). In ACRIN validation data, PLCO2012results demonstrated good calibration. Individuals who had initial negative scans but elevated PLCOm2012 six-year risks of at least 2.6% did not have risks decline below the 1.5% screening eligibility criterion when subsequent screens were negative.
According to this analysis, some individuals with elevated risk scores who have negative initial screens remain at elevated risks, warranting annual screening. Positive screens seem to increase baseline risk scores and may identify high-risk individuals for continued screening and enrollment into clinical trials.
ClinicalTrials.gov Identifier: NCT00047385.
低剂量计算机断层扫描肺癌筛查在应用于高危人群时最有效。
开发和验证一种包含低剂量计算机断层扫描筛查结果的风险预测模型。
设计、地点和参与者:在全国肺癌筛查试验(NLST)肺筛查研究(LSS)数据中开发了逻辑回归风险模型,并在 NLST 美国放射学院成像网络(ACRIN)数据中进行了验证。NLST 是一项随机临床试验,于 2002 年 8 月至 2004 年 4 月间招募参与者,随访至 2009 年 12 月 31 日。对 NLST 数据的二次分析于 2013 年 8 月 10 日至 2018 年 11 月 1 日进行。包括 LSS(n=14576)和 ACRIN(n=7653)参与者,他们进行了 3 次筛查,随访时间充足,且有完整的预测因子信息。
第三次筛查后 1 至 4 年内发生的肺癌(LSS 202 例,ACRIN 96 例)。预测因子包括经过验证的 PLCOm2012 风险模型和 Lung CT Screening Reporting & Data System(Lung-RADS)筛查结果的分数。
在 22229 名参与者中,总体平均(标准差)年龄为 61.3(5.0)岁,59.3%为男性,90.9%为非西班牙裔白人。在随访期间,22229 人中诊断出 298 例肺癌(1.3%)。根据相似的关联,将 8 种结果组合合并为 4 组。与 3 次阴性筛查的参与者相比,调整 PLCOm2012 风险后,1 次阳性筛查和最后 1 次阴性筛查的参与者比值比为 1.93(95%CI,1.34-2.76),而 2 次阳性筛查和最后 1 次阴性或 2 次阴性筛查和最后 1 次阳性筛查的参与者比值比为 2.66(95%CI,1.60-4.43);当 2 次或更多次筛查结果阳性且最后一次结果为阳性时,比值比为 8.97(95%CI,5.76-13.97)。在 ACRIN 验证数据中,包含 PLCOm2012 评分和筛查结果(PLCO2012results)的模型显示出显著更高的区分度(曲线下面积,0.761;95%CI,0.716-0.799),而排除筛查结果(PLCOm2012)时的曲线下面积(0.687;95%CI,0.645-0.728)(P<0.001)。在 ACRIN 验证数据中,PLCO2012results 显示出良好的校准度。初始阴性扫描但 PLCOm2012 六年后风险至少为 2.6%的个体,当后续筛查结果为阴性时,其风险不会降至 1.5%的筛查资格标准以下。
根据该分析,一些风险评分升高但初始筛查结果为阴性的个体仍处于较高风险,需要每年进行筛查。阳性筛查似乎会增加基线风险评分,并可能识别出需要继续筛查和入组临床试验的高危个体。
ClinicalTrials.gov 标识符:NCT00047385。