Núñez David Aramburu, Lu Yonggang, Paudyal Ramesh, Hatzoglou Vaios, Moreira Andre L, Oh Jung Hun, Stambuk Hilda E, Mazaheri Yousef, Gonen Mithat, Ghossein Ronald A, Shaha Ashok R, Tuttle R Michael, Shukla-Dave Amita
Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY.
Department of Radiology, Medical College of Wisconsin, Milwaukee, WI.
Tomography. 2019 Mar;5(1):26-35. doi: 10.18383/j.tom.2018.00054.
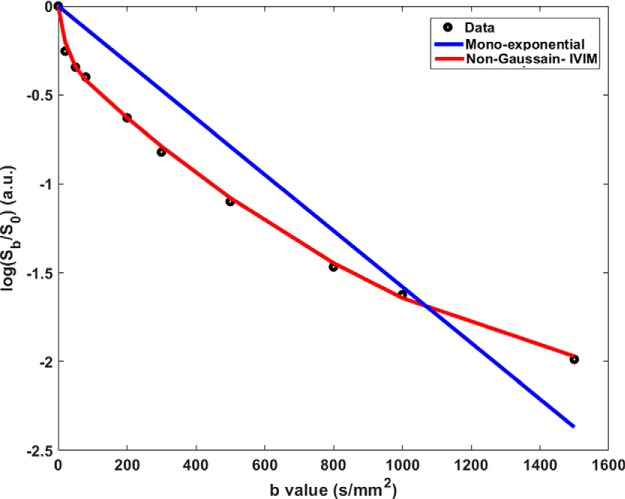
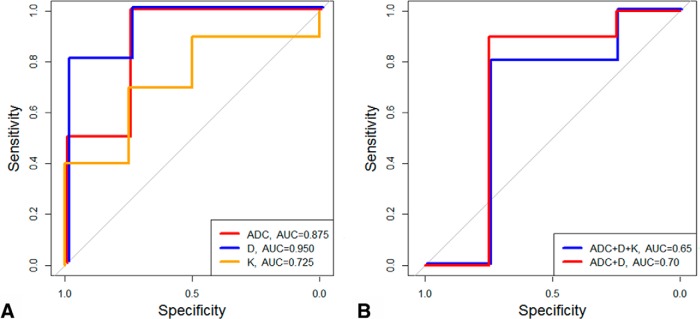
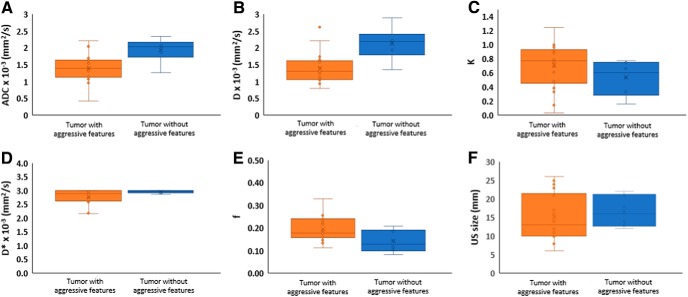
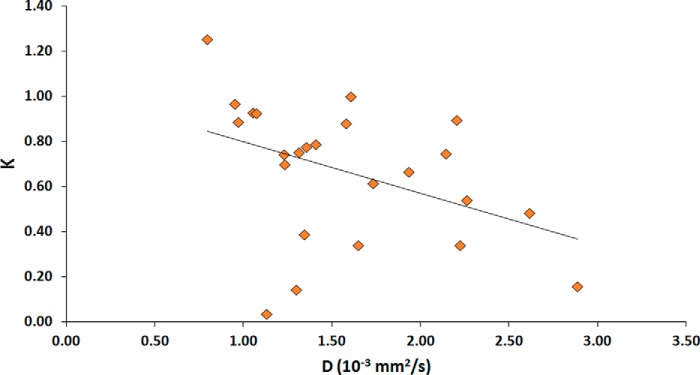
We assessed a priori aggressive features using quantitative diffusion-weighted imaging metrics to preclude an active surveillance management approach in patients with papillary thyroid cancer (PTC) with tumor size 1-2 cm. This prospective study enrolled 24 patients with PTC who underwent pretreatment multi-b-value diffusion-weighted imaging on a GE 3 T magnetic resonance imaging scanner. The apparent diffusion coefficient (ADC) metric was calculated from monoexponential model, and the perfusion fraction (), diffusion coefficient (), pseudo-diffusion coefficient (), and diffusion kurtosis coefficient () metrics were estimated using the non-Gaussian intravoxel incoherent motion model. Neck ultrasonography examination data were used to calculate tumor size. The receiver operating characteristic curve assessed the discriminative specificity, sensitivity, and accuracy between PTCs with and without features of tumor aggressiveness. Multivariate logistic regression analysis was performed on metrics using a leave-1-out cross-validation method. Tumor aggressiveness was defined by surgical histopathology. Tumors with aggressive features had significantly lower ADC and values than tumors without tumor-aggressive features ( < .05). The absolute relative change was 46% in metric value between the 2 tumor types. In total, 14 patients were in the critical size range (1-2 cm) measured by ultrasonography, and the ADC and were significantly different and able to differentiate between the 2 tumor types ( < .05). ADC and can distinguish tumors with aggressive histological features to preclude an active surveillance management approach in patients with PTC with tumors measuring 1-2 cm.
我们使用定量扩散加权成像指标对具有先验侵袭性特征进行评估,以排除肿瘤大小为1 - 2 cm的甲状腺乳头状癌(PTC)患者采用主动监测管理方法的可能性。这项前瞻性研究纳入了24例接受PTC治疗的患者,这些患者在GE 3 T磁共振成像扫描仪上进行了预处理多b值扩散加权成像。表观扩散系数(ADC)指标由单指数模型计算得出,灌注分数()、扩散系数()、伪扩散系数()和扩散峰度系数()指标使用非高斯体素内不相干运动模型进行估计。颈部超声检查数据用于计算肿瘤大小。受试者工作特征曲线评估了具有和不具有肿瘤侵袭性特征的PTC之间的鉴别特异性、敏感性和准确性。使用留一法交叉验证方法对指标进行多变量逻辑回归分析。肿瘤侵袭性由手术组织病理学定义。具有侵袭性特征的肿瘤的ADC和值显著低于无肿瘤侵袭性特征的肿瘤(<0.05)。两种肿瘤类型之间的指标值绝对相对变化为46%。总共有14例患者处于超声测量的临界大小范围(1 - 2 cm),ADC和存在显著差异,能够区分这两种肿瘤类型(<0.05)。ADC和能够区分具有侵袭性组织学特征的肿瘤,以排除肿瘤大小为1 - 2 cm的PTC患者采用主动监测管理方法的可能性。