Advancing New Standards in Reproductive Health (ANSIRH), Department of Obstetrics, Gynecology, and Reproductive Sciences, University of California, San Francisco, Oakland, California.
Pacific Institute for Research and Evaluation (PIRE), Santa Cruz, California.
Womens Health Issues. 2019 May-Jun;29(3):213-221. doi: 10.1016/j.whi.2019.02.001. Epub 2019 Mar 12.
Most states have at least one policy targeting alcohol use during pregnancy. The public health impact of these policies has not been examined. We sought to examine the relationship between state-level policies targeting alcohol use during pregnancy and alcohol use among pregnant women.
Data include state-level alcohol and pregnancy policy data and individual-level U.S. Behavioral Risk Factor Surveillance System data about pregnant women's alcohol use from 1985 to 2016 (N = 57,194). Supportive policies include mandatory warning signs, priority substance abuse treatment, reporting requirements for data and treatment purposes, and prohibitions on criminal prosecution. Punitive policies include civil commitment, Child Protective Services reporting requirements, and child abuse/neglect. Analyses include logistic regression models that adjust for individual- and state-level controls, include fixed effects for state and year, account for clustering by state, and weight by probability of selection.
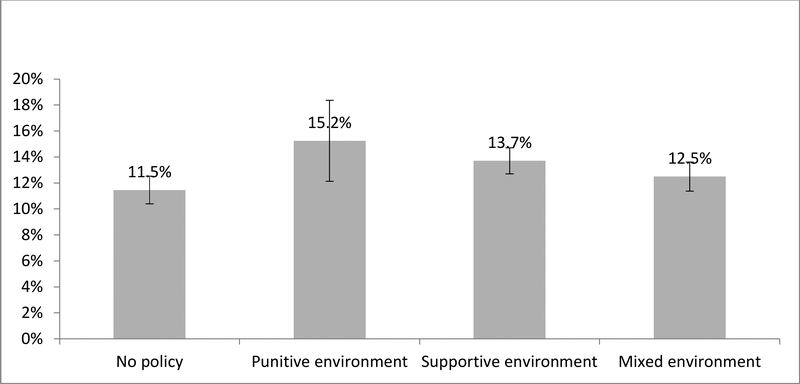
Relative to having no policies, supportive policy environments were associated with more any drinking, but not binge or heavy drinking. Of individual supportive policies, only the following relationships were statistically significant: mandatory warning signs was associated with lower odds of binge drinking, and priority treatment for pregnant women and women with children was associated with higher odds of any drinking. Relative to no policies, punitive policy environments were also associated with more drinking, but not with binge or heavy drinking. Of individual punitive policies, only child abuse/neglect was associated with lower odds of binge and heavy drinking. Mixed policy environments were not associated with any alcohol outcome.
Most policies targeting alcohol use during pregnancy do not seem to be associated with less alcohol consumption during pregnancy.
大多数州都至少有一项针对孕期饮酒的政策。但这些政策的公共卫生影响尚未得到检验。我们旨在探讨州级孕期饮酒政策与孕妇饮酒行为之间的关系。
数据包括州级酒精与妊娠政策数据以及 1985 年至 2016 年期间全美行为风险因素监测系统关于孕妇饮酒行为的个人层面数据(N=57194)。支持性政策包括强制性警示标志、优先物质滥用治疗、数据和治疗目的报告要求,以及禁止刑事起诉。惩罚性政策包括民事拘留、儿童保护服务报告要求和虐待/忽视儿童。分析包括调整个体和州级控制因素的逻辑回归模型,包括州和年份的固定效应,考虑州聚类,以及按选择概率加权。
与没有政策相比,支持性政策环境与更多的任何饮酒有关,但与狂饮或重度饮酒无关。在个体支持性政策中,只有以下关系具有统计学意义:强制性警示标志与狂饮的几率降低有关,而孕妇和有子女的妇女的优先治疗与任何饮酒的几率增加有关。与没有政策相比,惩罚性政策环境也与更多的饮酒有关,但与狂饮或重度饮酒无关。在个体惩罚性政策中,只有虐待/忽视儿童与狂饮和重度饮酒的几率降低有关。混合政策环境与任何酒精摄入结果均无关。
大多数针对孕期饮酒的政策似乎并未与孕期饮酒量减少相关。