Department of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands.
Departmesnt of Neurosurgery, University Medical Center Utrecht, Internal Postage G03.124, PO-box 85500, 3584 CX, Utrecht, The Netherlands.
Acta Neurochir (Wien). 2019 May;161(5):865-870. doi: 10.1007/s00701-019-03867-8. Epub 2019 Mar 16.
In the past, the accuracy of surface matching has been shown to be disappointing. We aimed to determine whether this had improved over the years by assessing application accuracy of current navigation systems, using either surface matching or point-pair matching.
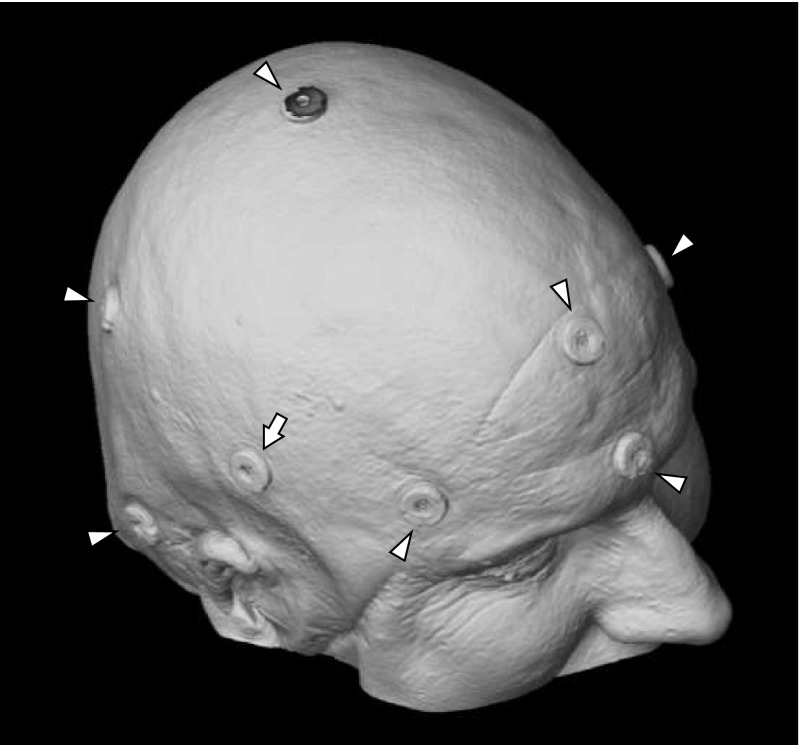
Eleven patients, scheduled for intracranial surgery, were included in this study after a power analysis had shown this small number to be sufficient. Prior to surgery, one additional fiducial marker was placed on the scalp, the "target marker," where the entry point of surgery was to be expected. Using one of three different navigation systems, two patient-to-image registration procedures were performed: one based on surface matching and one based on point-pair matching. Each registration procedure was followed by the digitization of the target marker's location, allowing calculation of the target registration error. If the system offered surface matching improvement, this was always used; and for the two systems that routinely offer an estimate of neuronavigation accuracy, this was also recorded.
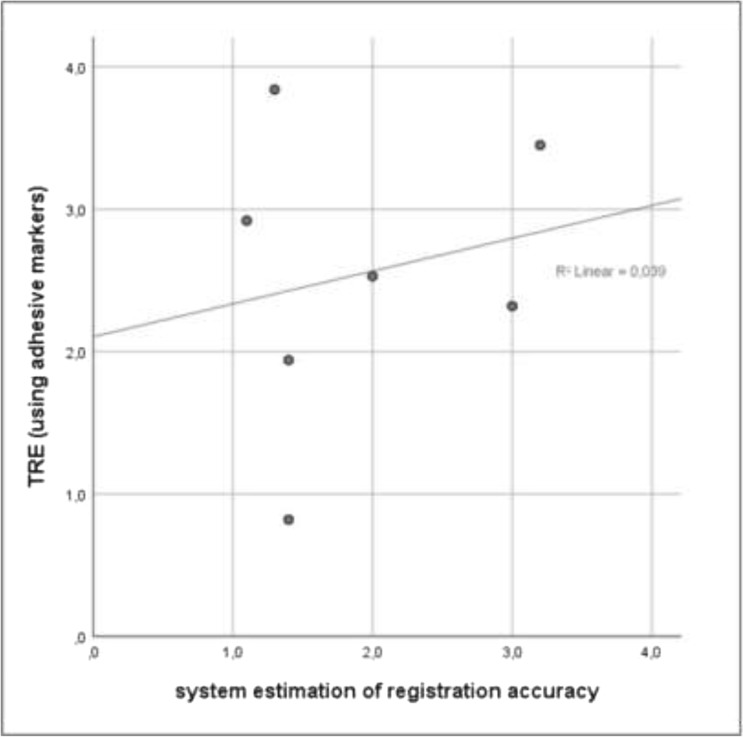
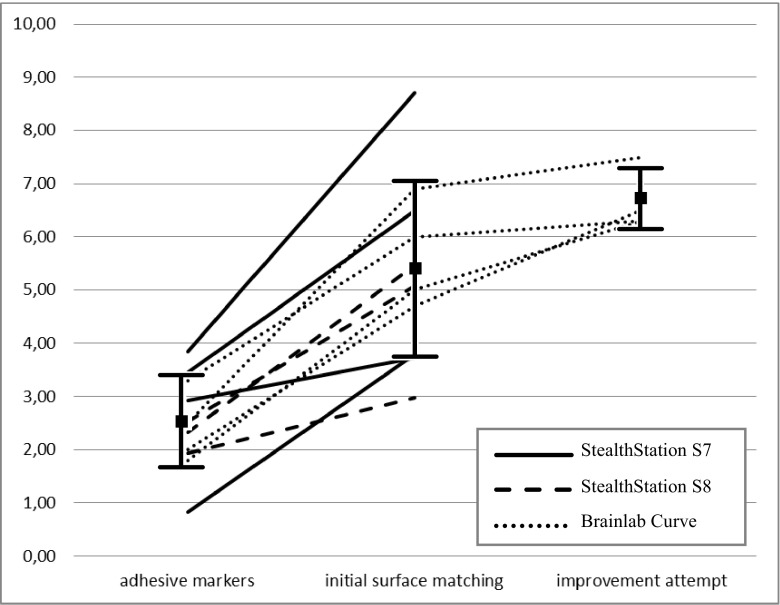
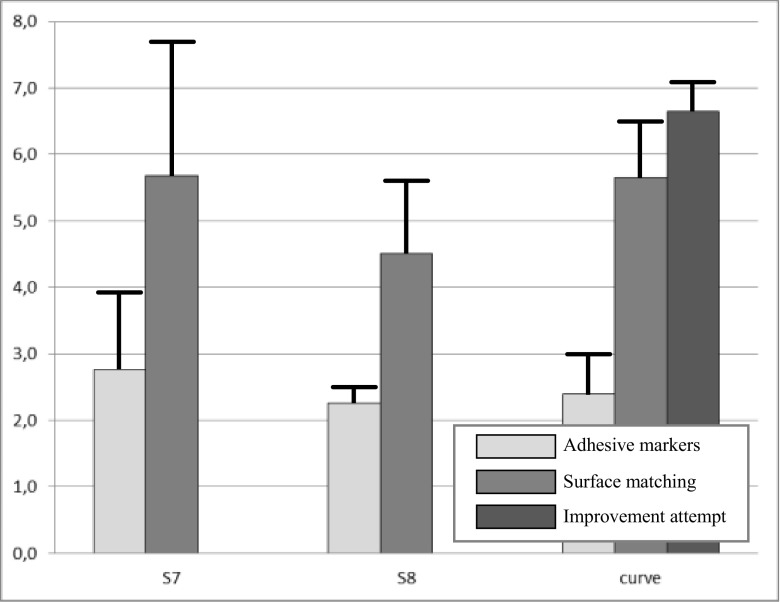
The error in localizing the target marker using point-pair matching or surface matching was respectively 2.49 mm and 5.35 mm, on average (p < 0.001). In those four cases where an attempt was made to improve the surface matching, the error increased to 6.35 mm, on average. For the seven cases where the system estimated accuracy, this estimate did not correlate with target registration error (R = 0.04, p = 0.67).
The accuracy of navigation systems has not improved over the last decade, with surface matching consistently yielding errors that are twice as large as when point-pair matching with adhesive markers is used. These errors are not reliably reflected by the systems own prediction, when offered. These results are important to make an informed choice between image-to-patient registration strategies, depending on the type of surgery at hand.
过去,表面匹配的准确性一直不尽如人意。我们旨在通过评估当前导航系统在应用中的准确性来确定这是否有所改善,这些系统分别使用表面匹配或点对匹配。
11 名计划接受颅内手术的患者参与了本研究,该研究通过一项功效分析表明,该小样本量足以得出结果。在手术前,头皮上额外放置了一个基准标记,即预计手术入口的“目标标记”。使用三种不同的导航系统中的一种,进行了两次基于患者图像的注册程序:一次基于表面匹配,一次基于点对匹配。每次注册程序后,都会对目标标记的位置进行数字化,从而计算目标注册误差。如果系统提供了表面匹配改进,将始终使用该改进;对于两个常规提供神经导航准确性估计的系统,也记录了该改进。
使用点对匹配或表面匹配定位目标标记的误差分别为 2.49 毫米和 5.35 毫米,平均而言(p<0.001)。在四个尝试改进表面匹配的病例中,误差平均增加到 6.35 毫米。在七个系统估计准确性的病例中,该估计与目标注册误差没有相关性(R=0.04,p=0.67)。
过去十年中,导航系统的准确性并未提高,表面匹配的误差始终是使用粘性标记进行点对匹配时的两倍。当系统提供时,这些误差不能可靠地反映其自身的预测。这些结果对于根据手头手术类型在图像到患者的注册策略之间做出明智的选择很重要。