Aramburu Amaia, Arostegui Inmaculada, Moraza Javier, Barrio Irantzu, Aburto Myriam, García-Loizaga Amaia, Uranga Ane, Zabala Txomin, Quintana José María, Esteban Cristóbal
Respiratory Department, Hospital Galdakao-Usansolo, Galdakao, Bizkaia, Spain,
Department of Applied Mathematics, Statistics and Operative Research, University of the Basque Country (UPV/EHU), Basque Country, Spain.
Int J Chron Obstruct Pulmon Dis. 2019 Mar 7;14:605-613. doi: 10.2147/COPD.S184695. eCollection 2019.
Our aim was to assess the impact of comorbidities on existing COPD prognosis scores.
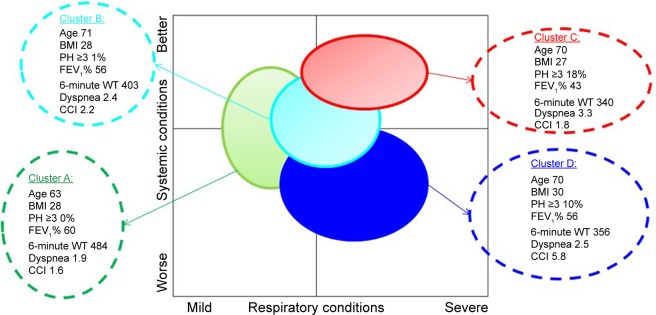
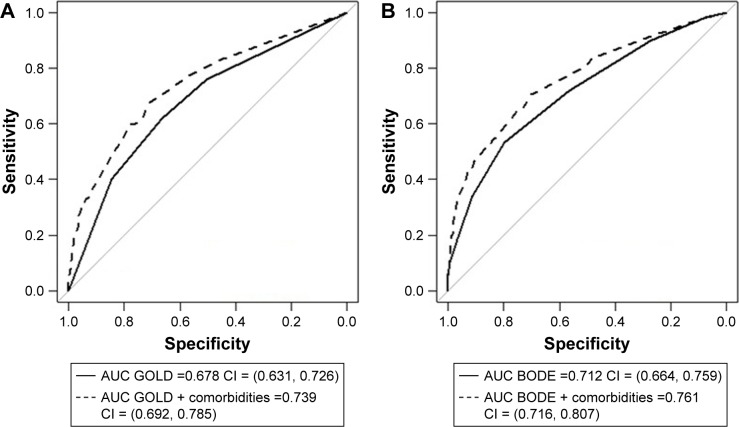
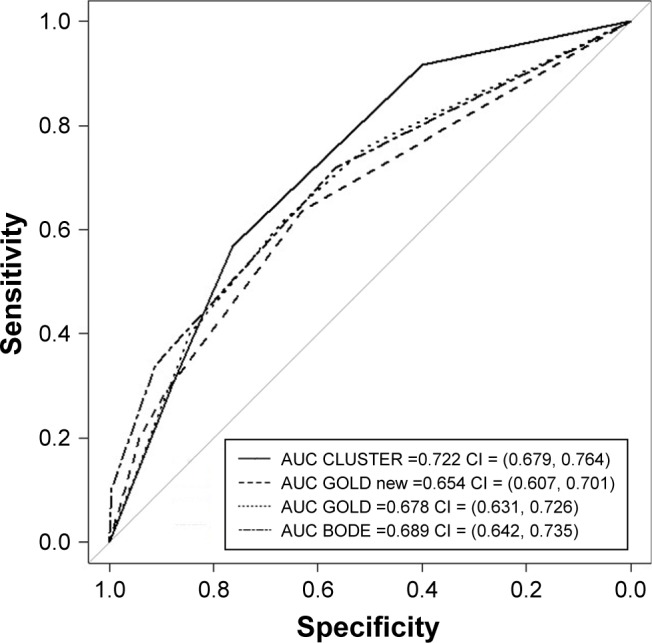
A total of 543 patients with COPD (FEV <80% and FEV/FVC <70%) were included between January 2003 and January 2004. Patients were stable for at least 6 weeks before inclusion and were followed for 5 years without any intervention by the research team. Comorbidities and causes of death were established from medical reports or information from primary care medical records. The GOLD system and the body mass index, obstruction, dyspnea and exercise (BODE) index were used for COPD classification. Patients were also classified into four clusters depending on the respiratory disease and comorbidities. Cluster analysis was performed by combining multiple correspondence analyses and automatic classification. Receiver operating characteristic curves and the area under the curve (AUC) were calculated for each model, and the DeLong test was used to evaluate differences between AUCs. Improvement in prediction ability was analyzed by the DeLong test, category-free net reclassification improvement and the integrated discrimination index.
Among the 543 patients enrolled, 521 (96%) were male, with a mean age of 68 years, mean body mass index 28.3 and mean FEV% 55%. A total of 167 patients died during the study follow-up. Comorbidities were prevalent in our cohort, with a mean Charlson index of 2.4. The most prevalent comorbidities were hypertension, diabetes mellitus and cardiovascular diseases. On comparing the BODE index, GOLD, GOLD and cluster analysis for predicting mortality, cluster system was found to be superior compared with GOLD (0.654 vs 0.722, =0.006), without significant differences between other classification models. When cardiovascular comorbidities and chronic renal failure were added to the existing scores, their prognostic capacity was statistically superior (<0.001).
Comorbidities should be taken into account in COPD management scores due to their prevalence and impact on mortality.
我们的目的是评估合并症对现有慢性阻塞性肺疾病(COPD)预后评分的影响。
2003年1月至2004年1月期间共纳入543例COPD患者(第1秒用力呼气容积[FEV]<80%且FEV/用力肺活量[FVC]<70%)。患者在纳入前至少稳定6周,且在研究团队未进行任何干预的情况下随访5年。合并症和死亡原因根据医疗报告或基层医疗记录中的信息确定。采用慢性阻塞性肺疾病全球倡议(GOLD)系统以及体重指数、气流受限、呼吸困难和运动(BODE)指数对COPD进行分类。根据呼吸系统疾病和合并症,患者还被分为四类。通过结合多重对应分析和自动分类进行聚类分析。计算每个模型的受试者工作特征曲线和曲线下面积(AUC),并使用德龙检验评估AUC之间的差异。通过德龙检验、无类别净重新分类改善和综合判别指数分析预测能力的改善情况。
在纳入的543例患者中,521例(96%)为男性,平均年龄68岁,平均体重指数28.标准3,平均FEV%为55%。在研究随访期间共有167例患者死亡。合并症在我们的队列中很常见,平均查尔森指数为2.4。最常见的合并症是高血压、糖尿病和心血管疾病。在比较BODE指数、GOLD、GOLD和聚类分析预测死亡率时,发现聚类系统优于GOLD(0.654对0.722,P=0.006),其他分类模型之间无显著差异。当将心血管合并症和慢性肾衰竭添加到现有评分中时,它们的预后能力在统计学上更优(P<0.001)。
由于合并症的普遍性及其对死亡率的影响,在COPD管理评分中应考虑合并症。