Department of Laboratory Medicine, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, China.
Department of Information Section, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, China.
J Transl Med. 2019 Mar 25;17(1):98. doi: 10.1186/s12967-019-1841-3.
Patients with HBsAg-positive gastric cancer (GC) are a heterogeneous group, and it is not possible to accurately predict the overall survival (OS) in these patients.
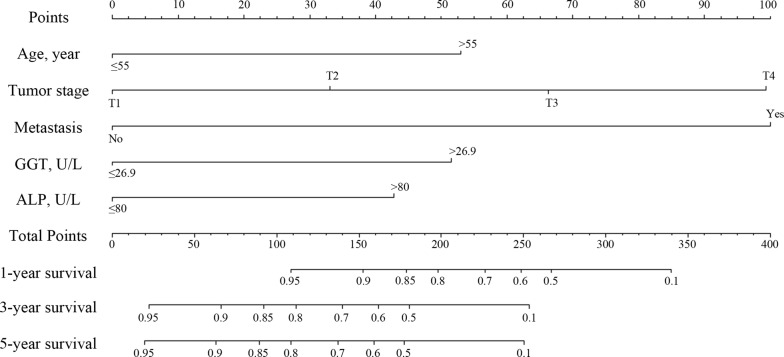
We developed and validated a nomogram to help improve prediction of OS in patients with HBsAg-positive GC. The nomogram was established by a development cohort (n = 245), and the validation cohort included 84 patients. Factors in the nomogram were identified by univariate and multivariate Cox hazard analysis. We tested the accuracy of the nomograms by discrimination and calibration, and plotted decision curves to assess the benefits of nomogram-assisted decisions in a clinical context. Then we evaluated the risk in the two cohort.
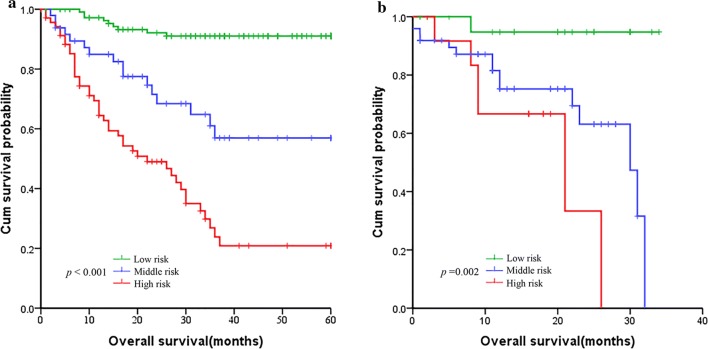
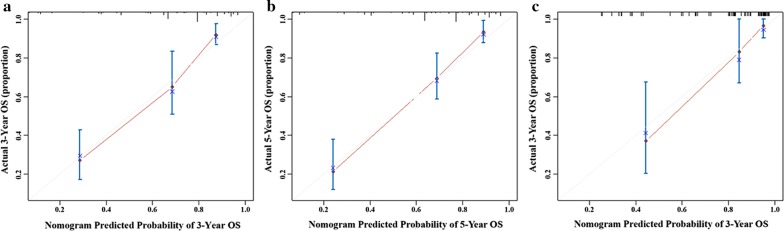
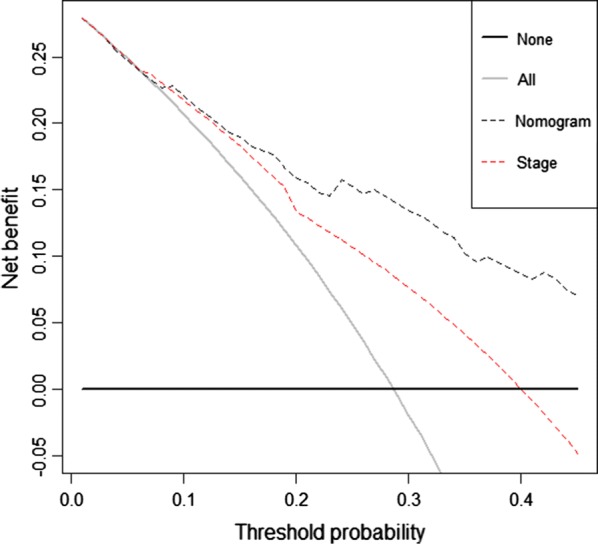
Significant predictors were age, tumor stage, distant metastases, gamma-glutamyl transpeptidase (GGT) and alkaline phosphatase (ALP). The proportional-hazards model (nomogram) was based on pre-treatment characteristics. The nomogram had a concordance index (C-index) of 0.812 (95% CI 0.762-0.862), which was superior than the C-index of AJCC TNM Stage (0.755, 95% CI 0.702-0.808). The calibration plot in the validation cohort based on 5 predictors suggested good agreement between actual and nomogram-predicted OS probabilities. The decision curve showed that the nomogram in predicting OS is better than that of TNM staging system in all range. Moreover, patients were divided into three distinct risk groups for OS by the nomogram: low risk group, middle risk group and high risk group, respectively.
This nomogram, using five pre-treatment characteristics, improves prediction of OS in patients with HBsAg-positive gastric cancer. It represents an improvement in prognostication over the current TNM stage. To generalize the use of this nomogram in other groups, additional validation with data from other institutions is required.
HBsAg 阳性胃癌(GC)患者是一个异质群体,无法准确预测这些患者的总生存期(OS)。
我们开发并验证了一个列线图,以帮助提高对 HBsAg 阳性 GC 患者 OS 的预测。该列线图由一个发展队列(n=245)建立,验证队列包括 84 名患者。通过单因素和多因素 Cox 风险分析确定列线图中的因素。我们通过区分度和校准来测试列线图的准确性,并绘制决策曲线,以评估在临床环境中使用列线图辅助决策的获益。然后我们评估了两个队列的风险。
显著的预测因素是年龄、肿瘤分期、远处转移、γ-谷氨酰转肽酶(GGT)和碱性磷酸酶(ALP)。基于治疗前特征的比例风险模型(列线图)。列线图的一致性指数(C 指数)为 0.812(95%CI 0.762-0.862),优于 AJCC TNM 分期的 C 指数(0.755,95%CI 0.702-0.808)。基于 5 个预测因素的验证队列校准图表明,实际和列线图预测 OS 概率之间存在良好的一致性。决策曲线表明,列线图在预测 OS 方面优于 TNM 分期系统,在所有范围内都有更好的效果。此外,根据列线图,患者被分为三个不同的 OS 风险组:低危组、中危组和高危组。
该列线图使用五个治疗前特征,可提高 HBsAg 阳性胃癌患者 OS 的预测。它在预后方面优于当前的 TNM 分期。为了将该列线图在其他人群中推广使用,需要用其他机构的数据进行额外验证。