Division of Epidemiology, Department of Medicine, Vanderbilt Epidemiology Center, Vanderbilt-Ingram Cancer Center, Vanderbilt University Medical Center, Nashville, Tennessee.
Division of Cancer Statistics Integration, Center for Cancer Control and Information Services, National Cancer Center, Tokyo, Japan.
JAMA Netw Open. 2019 Mar 1;2(3):e191474. doi: 10.1001/jamanetworkopen.2019.1474.
Understanding birth cohort-specific tobacco smoking patterns and their association with total and cause-specific mortality is important for projecting future deaths due to tobacco smoking across Asian populations.
To assess secular trends of tobacco smoking by countries or regions and birth cohorts and evaluate the consequent mortality in Asian populations.
DESIGN, SETTING, AND PARTICIPANTS: This pooled meta-analysis was based on individual participant data from 20 prospective cohort studies participating in the Asia Cohort Consortium. Between September 1, 2017, and March 31, 2018, a total of 1 002 258 Asian individuals 35 years or older were analyzed using Cox proportional hazards regression analysis and random-effects meta-analysis. The pooled results were presented for mainland China; Japan; Korea, Singapore, and Taiwan; and India.
Tobacco use status, age at starting smoking, number of cigarettes smoked per day, and age at quitting smoking.
Country or region and birth cohort-specific mortality and the population attributable risk for deaths from all causes and from lung cancer.
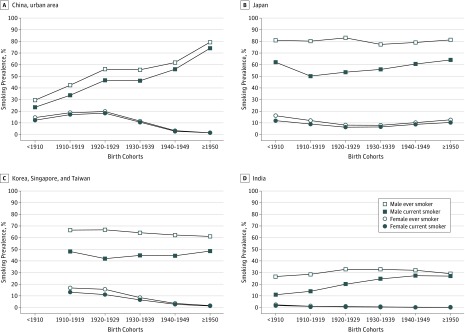
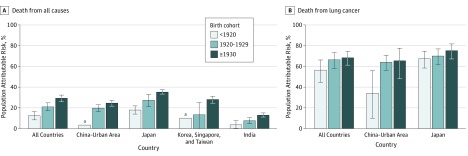
Of 1 002 258 participants (51.1% women and 48.9% men; mean [SD] age at baseline, 54.6 [10.4] years), 144 366 deaths (9158 deaths from lung cancer) were ascertained during a mean (SD) follow-up of 11.7 (5.3) years. Smoking prevalence for men steadily increased in China and India, whereas it plateaued in Japan and Korea, Singapore, and Taiwan. Among Asian male smokers, the mean age at starting smoking decreased in successive birth cohorts, while the mean number of cigarettes smoked per day increased. These changes were associated with an increasing relative risk of death in association with current smoking in successive birth cohorts of pre-1920, 1920s, and 1930 or later, with hazard ratios for all-cause mortality of 1.26 (95% CI, 1.17-1.37) for the pre-1920 birth cohort, 1.47 (95% CI, 1.35-1.61) for the 1920s birth cohort, and 1.70 (95% CI, 1.57-1.84) for the cohort born in 1930 or later. The hazard ratios for lung cancer mortality were 3.38 (95% CI, 2.25-5.07) for the pre-1920 birth cohort, 4.74 (95% CI, 3.56-6.32) for the 1920s birth cohort, and 4.80 (95% CI, 3.71-6.19) for the cohort born in 1930 or later. Tobacco smoking accounted for 12.5% (95% CI, 8.4%-16.3%) of all-cause mortality in the pre-1920 birth cohort, 21.1% (95% CI, 17.3%-24.9%) of all-cause mortality in the 1920s birth cohort, and 29.3% (95% CI, 26.0%-32.3%) of all-cause mortality for the cohort born in 1930 or later. Tobacco smoking among men accounted for 56.6% (95% CI, 44.7%-66.3%) of lung cancer mortality in the pre-1920 birth cohort, 66.6% (95% CI, 58.3%-73.5%) of lung cancer mortality in the 1920s birth cohort, and 68.4% (95% CI, 61.3%-74.4%) of lung cancer mortality for the cohort born in 1930 or later. For women, tobacco smoking patterns and lung cancer mortality varied substantially by countries and regions.
In this study, mortality associated with tobacco smoking continued to increase among Asian men in recent birth cohorts, indicating that tobacco smoking will remain a major public health problem in most Asian countries in the coming decades. Implementing comprehensive tobacco-control programs is warranted to end the tobacco epidemic.
了解特定于出生队列的吸烟模式及其与全因和特定原因死亡率的关联对于预测亚洲人群因吸烟导致的未来死亡人数非常重要。
评估亚洲国家或地区和出生队列的烟草使用趋势,并评估其随后的死亡率。
设计、设置和参与者:本汇总荟萃分析基于 20 项参与亚洲队列联盟的前瞻性队列研究的个体参与者数据。在 2017 年 9 月 1 日至 2018 年 3 月 31 日期间,使用 Cox 比例风险回归分析和随机效应荟萃分析对 35 岁或以上的 1002258 名亚洲人进行了分析。汇总结果分别呈现给中国大陆、日本、韩国、新加坡和中国台湾以及印度。
吸烟状况、开始吸烟的年龄、每天吸烟的支数和戒烟年龄。
全因和肺癌死亡率以及归因于所有原因和肺癌死亡的人群归因风险的国家或地区和出生队列特异性。
在 1002258 名参与者中(51.1%为女性,48.9%为男性;基线时的平均[标准差]年龄为 54.6[10.4]岁),在平均(标准差)随访 11.7(5.3)年后,共确定了 144366 例死亡(9158 例死于肺癌)。在中国和印度,男性吸烟率稳步上升,而在日本和韩国、新加坡和中国台湾,吸烟率则趋于平稳。在亚洲男性吸烟者中,开始吸烟的平均年龄在连续出生队列中逐渐下降,而每天吸烟的平均支数增加。这些变化与当前吸烟的连续出生队列中与死亡相关的相对风险增加相关,1920 年前、1920 年代和 1930 年或以后出生的队列的全因死亡率的危险比分别为 1.26(95%CI,1.17-1.37)、1.47(95%CI,1.35-1.61)和 1.70(95%CI,1.57-1.84)。肺癌死亡率的危险比分别为 3.38(95%CI,2.25-5.07)、4.74(95%CI,3.56-6.32)和 4.80(95%CI,3.71-6.19)。1920 年前出生的队列、1920 年代出生的队列和 1930 年或以后出生的队列。吸烟导致 1920 年前出生的队列全因死亡率的 12.5%(95%CI,8.4%-16.3%)、1920 年代出生的队列全因死亡率的 21.1%(95%CI,17.3%-24.9%)和 1930 年或以后出生的队列全因死亡率的 29.3%(95%CI,26.0%-32.3%)。男性吸烟导致 1920 年前出生的队列肺癌死亡率的 56.6%(95%CI,44.7%-66.3%)、1920 年代出生的队列肺癌死亡率的 66.6%(95%CI,58.3%-73.5%)和 1930 年或以后出生的队列肺癌死亡率的 68.4%(95%CI,61.3%-74.4%)。对于女性,吸烟模式和肺癌死亡率在不同国家和地区有很大差异。
在这项研究中,亚洲男性中与吸烟相关的死亡率在最近的出生队列中继续上升,这表明在未来几十年,吸烟仍将是大多数亚洲国家的主要公共卫生问题。实施全面的烟草控制计划是必要的,以结束烟草流行。