Poverty, Health and Nutrition Division, The International Food Policy Research Institute, 2001 K Street NW, Washington DC, 20005, United States of America.
Bull World Health Organ. 2019 Apr 1;97(4):270-282. doi: 10.2471/BLT.18.221135. Epub 2019 Feb 25.
To investigate coverage and equity of India's Integrated Child Development Services programme across the continuum of care from pregnancy to early childhood, before and after the programme was expanded to provide universal access.
The programme offers nutrition and health services to pregnant and lactating mothers and young children. We used data from nationally representative surveys in 2005-2006 and 2015-2016, including 36 850 mother-child pairs in 2006 and 190 804 in 2016. We assessed changes in the equity of use of programme services by socioeconomic quintile, caste, education and rural or urban residence. We used regression models to investigate the determinants of programme use.
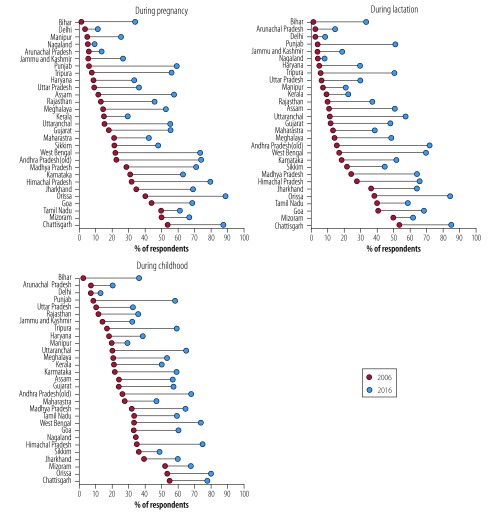
The mean proportion of respondents using programme services increased between 2006 and 2016, from 9.6% to 37.9% for supplementary food, 3.2% to 21.0% for health and nutrition education, 4.5% to 28% for health check-ups and 10.4% to 24.2% for child-specific services (e.g. immunization, growth monitoring). Wealth, maternal education and caste showed the largest positive associations with use of services. However, expansion in service use varied at the sub-national level. Although overall use had improved and reached marginalized groups such as disadvantaged castes and tribes, the poorest quintiles of the population were still left behind, especially in the largest states that carry the highest burden of undernutrition.
India's policy reforms have increased coverage of the programme at the national level, including for marginalized groups. With further scaling-up, the programme needs to focus on reaching households from the lowest socioeconomic strata and women with low schooling levels.
调查印度综合儿童发展服务计划(ICDS)在扩大服务范围以实现普及之前和之后,在从怀孕到幼儿的整个照护过程中的覆盖范围和公平性。
该计划为孕妇和哺乳期妇女以及幼儿提供营养和健康服务。我们使用了 2005-2006 年和 2015-2016 年全国代表性调查的数据,包括 2006 年的 36850 对母婴和 2016 年的 190804 对母婴。我们评估了按社会经济五分位数、种姓、教育和农村或城市居住情况划分的方案服务使用公平性的变化。我们使用回归模型来研究方案使用的决定因素。
2006 年至 2016 年间,使用方案服务的受访者比例平均有所增加,从补充食品的 9.6%增加到 37.9%,从健康和营养教育的 3.2%增加到 21.0%,从健康检查的 4.5%增加到 28%,从儿童特定服务(如免疫、生长监测)的 10.4%增加到 24.2%。财富、母亲教育和种姓与服务使用之间存在最大的正相关关系。然而,服务使用的扩大在国家以下一级存在差异。尽管总体使用率有所提高,并且已经覆盖了弱势种姓和部落等边缘化群体,但最贫穷的五分之一人口仍被抛在后面,尤其是在营养不足负担最重的最大邦。
印度的政策改革提高了全国范围内(包括边缘化群体)该计划的覆盖率。随着进一步扩大规模,该计划需要关注来自社会经济地位最低阶层和教育水平较低的妇女的家庭。