Abramson Cancer Center, University of Pennsylvania, Philadelphia, Pennsylvania, USA
Leonard Davis Institute, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Oncologist. 2019 Jun;24(6):e397-e399. doi: 10.1634/theoncologist.2019-0039. Epub 2019 Apr 3.
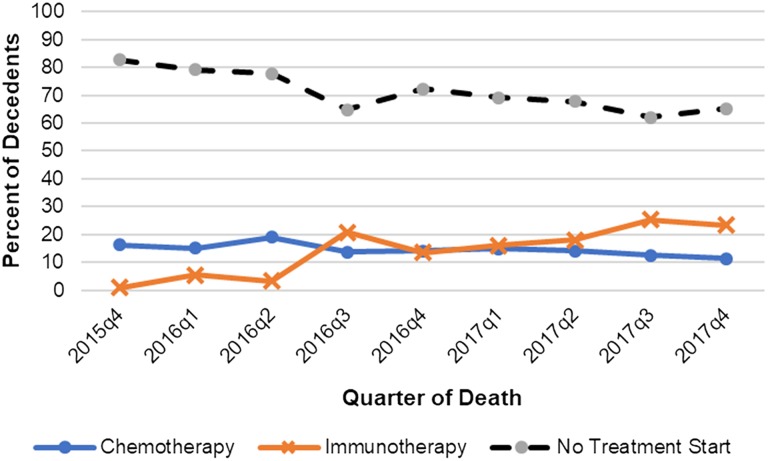
Several immune checkpoint inhibitor therapies (CPIs) have been approved to treat metastatic urothelial cell carcinoma (mUC). Because of the favorable toxicity profile of CPI compared with chemotherapy, oncologists may have a low threshold to prescribe CPI to patients near the end of life. We evaluated trends in initiation of end-of-life systemic therapy in 1,637 individuals in the Flatiron Health Database who were diagnosed with mUC between 2015 and 2017 and who died. Rates of systemic therapy initiation in the last 30 and 60 days of life were 17.0% and 29.8%, respectively. The quarterly proportion of patients who initiated CPI within 60 days of death increased from 1.0% to 23% during the study period ( < .001). After CPI approval, end-of-life CPI initiation significantly increased among patients with poor performance status ( = .020) and did not significantly change among individuals with good performance status. The quarterly proportion of patients who initiated any systemic therapy at the end of life doubled (17.4% to 34.8%) during the study period, largely explained by increased CPI use. These findings suggest a dramatic rise in CPI use at the end of life in patients with mUC, a finding that may have important guideline and policy implications.
几种免疫检查点抑制剂疗法(CPIs)已被批准用于治疗转移性尿路上皮细胞癌(mUC)。由于 CPI 与化疗相比具有良好的毒性特征,因此肿瘤学家可能会降低门槛,为生命末期的患者开 CPI 处方。我们评估了 2015 年至 2017 年间在 Flatiron Health 数据库中被诊断为 mUC 并死亡的 1637 名个体中临终系统治疗开始的趋势。在生命的最后 30 天和 60 天内开始系统治疗的比率分别为 17.0%和 29.8%。在研究期间,在死亡后 60 天内开始 CPI 的患者每季度比例从 1.0%增加到 23%(<0.001)。在 CPI 获得批准后,在表现状态较差的患者中,临终 CPI 开始显著增加(=0.020),而在表现状态良好的个体中则没有明显变化。在研究期间,在生命末期开始任何系统治疗的患者每季度比例增加了一倍(从 17.4%增加到 34.8%),这主要归因于 CPI 使用的增加。这些发现表明,在 mUC 患者的生命末期 CPI 的使用急剧增加,这一发现可能对指南和政策具有重要意义。