Instituto do Coração (InCor), São Paulo, SP - Brazil.
Department of Cardiology and Pneumology - University of Göttingen Medical Centre, Göttingen - Germany.
Arq Bras Cardiol. 2019 Jun;112(6):739-746. doi: 10.5935/abc.20190061. Epub 2019 Apr 8.
Resting sympathetic hyperactivity and impaired parasympathetic reactivation after exercise have been described in patients with heart failure (HF). However, the association of these autonomic changes in patients with HF and sarcopenia is unknown.
The aim of this study was to evaluate the impact of autonomic modulation on sarcopenia in male patients with HF.
We enrolled 116 male patients with HF and left ventricular ejection fraction < 40%. All patients underwent a maximal cardiopulmonary exercise testing. Maximal heart rate was recorded and delta heart rate recovery (∆HRR) was assessed at 1st and 2nd minutes after exercise. Muscle sympathetic nerve activity (MSNA) was recorded by microneurography. Dual-energy X-ray absorptiometry was used to measure body composition and sarcopenia was defined by the sum of appendicular lean muscle mass (ALM) divided by height in meters squared and handgrip strength.
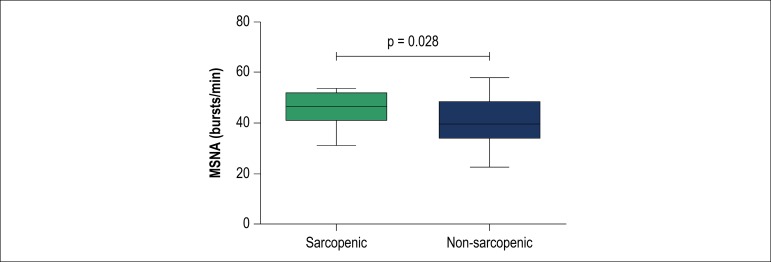
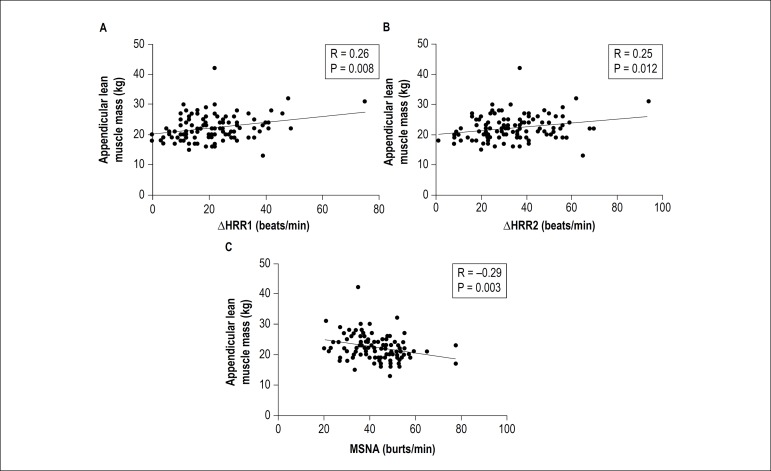
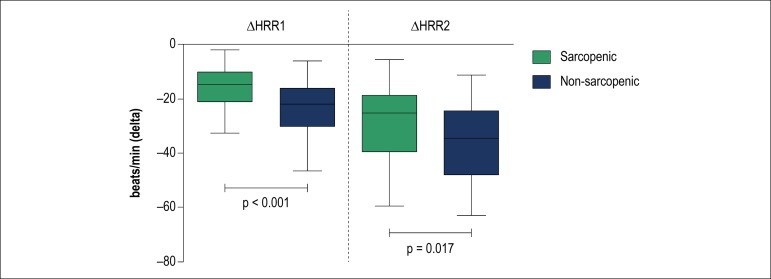
Sarcopenia was identified in 33 patients (28%). Patients with sarcopenia had higher MSNA than those without (47 [41-52] vs. 40 [34-48] bursts/min, p = 0.028). Sarcopenic patients showed lower ∆HRR at 1st (15 [10-21] vs. 22 [16-30] beats/min, p < 0.001) and 2nd min (25 [19-39] vs. 35 [24-48] beats/min, p = 0.017) than non-sarcopenic. There was a positive correlation between ALM and ∆HRR at 1st (r = 0.26, p = 0.008) and 2nd min (r = 0.25, p = 0.012). We observed a negative correlation between ALM and MSNA (r = -0.29, p = 0.003).
Sympatho-vagal imbalance seems to be associated with sarcopenia in male patients with HF. These results highlight the importance of a therapeutic approach in patients with muscle wasting and increased peripheral sympathetic outflow.
在心力衰竭(HF)患者中,已经描述了运动后休息时交感神经活性亢进和副交感神经重新激活受损。然而,HF 患者中这些自主神经变化与肌肉减少症的关系尚不清楚。
本研究旨在评估自主神经调节对男性 HF 患者肌肉减少症的影响。
我们纳入了 116 名左心室射血分数<40%的男性 HF 患者。所有患者均进行了最大心肺运动测试。记录最大心率,并在运动后 1 分钟和 2 分钟评估心率恢复的差值(∆HRR)。通过微神经记录肌间神经活动(MSNA)。双能 X 线吸收法用于测量身体成分,肌肉减少症定义为四肢瘦体重(ALM)除以身高的平方和握力。
33 名患者(28%)存在肌肉减少症。与无肌肉减少症的患者相比,存在肌肉减少症的患者 MSNA 更高(47[41-52] 与 40[34-48] 次/分,p=0.028)。肌肉减少症患者在第 1 分钟(15[10-21] 与 22[16-30] 次/分,p<0.001)和第 2 分钟(25[19-39] 与 35[24-48] 次/分,p=0.017)的 ∆HRR 较低。ALM 与第 1 分钟(r=0.26,p=0.008)和第 2 分钟(r=0.25,p=0.012)的 ∆HRR 呈正相关。我们观察到 ALM 与 MSNA 呈负相关(r=-0.29,p=0.003)。
交感神经-迷走神经失衡似乎与 HF 男性患者的肌肉减少症有关。这些结果强调了在肌肉减少症和外周交感神经输出增加的患者中进行治疗的重要性。