Department of Internal Medicine, Infectious Disease Unit, Niger Delta University Teaching Hospital, Okolobiri, Bayelsa State, Nigeria.
Nigerian Centre for Disease Control, Abuja, Nigeria.
PLoS One. 2019 Apr 17;14(4):e0214229. doi: 10.1371/journal.pone.0214229. eCollection 2019.
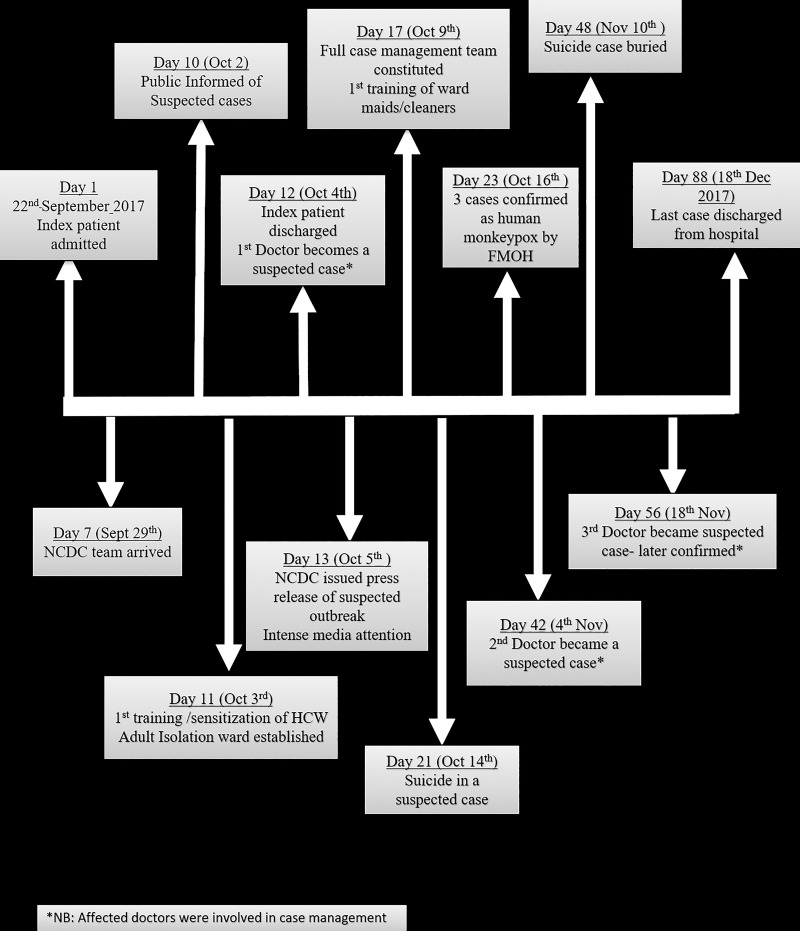
In September 2017, Nigeria experienced a large outbreak of human monkeypox (HMPX). In this study, we report the outbreak experience and response in the Niger Delta University Teaching Hospital (NDUTH), Bayelsa state, where the index case and majority of suspected cases were reported.
In a cross-sectional study between September 25th and 31st December 2017, we reviewed the clinical and laboratory characteristics of all suspected and confirmed cases of HMPX seen at the NDUTH and appraised the plans, activities and challenges of the hospital in response to the outbreak based on documented observations of the hospital's infection control committee (IPC). Monkeypox cases were defined using the interim national guidelines as provided by the Nigerian Centre for Disease Control (NCDC).
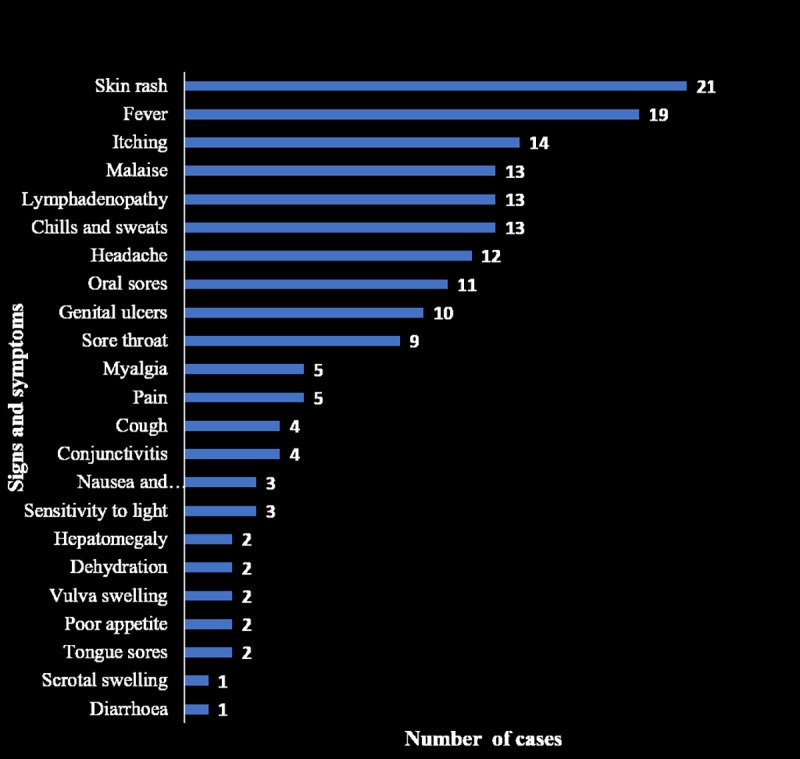
Of 38 suspected cases of HMPX, 18(47.4%) were laboratory confirmed, 3(7.9%) were probable, while 17 (18.4%) did not fit the case definition for HMPX. Majority of the confirmed/probable cases were adults (80.9%) and males (80.9%). There was concomitant chicken pox, syphilis and HIV-1 infections in two confirmed cases and a case of nosocomial infection in one healthcare worker (HCW). The hospital established a make-shift isolation ward for case management, constituted a HMPX response team and provided IPC resources. At the outset, some HCWs were reluctant to participate in the outbreak and others avoided suspected patients. Some patients and their family members experienced stigma and discrimination and there were cases of refusal of isolation. Repeated trainings and collaborative efforts by all stakeholders addressed some of these challenges and eventually led to successful containment of the outbreak.
While the 2017 outbreak of human monkeypox in Nigeria was contained, our report reveals gaps in outbreak response that could serve as lessons to other hospitals to strengthen epidemic preparedness and response activities in the hospital setting.
2017 年 9 月,尼日利亚发生了大规模的人类猴痘(HMPX)疫情。在本研究中,我们报告了在尼日尔三角洲大学教学医院(NDUTH)发生的疫情经验和应对情况,该医院报告了首例病例和大多数疑似病例。
在 2017 年 9 月 25 日至 12 月 31 日期间进行的一项横断面研究中,我们回顾了在 NDUTH 就诊的所有疑似和确诊的人类猴痘病例的临床和实验室特征,并根据医院感染控制委员会(IPC)的记录观察,评估了医院对疫情的应对计划、活动和挑战。猴痘病例的定义使用尼日利亚疾病控制中心(NCDC)提供的临时国家指南。
在 38 例疑似人类猴痘病例中,18 例(47.4%)经实验室确诊,3 例(7.9%)为可能病例,17 例(18.4%)不符合人类猴痘病例定义。大多数确诊/可能病例为成年人(80.9%)和男性(80.9%)。在 2 例确诊病例中同时存在水痘、梅毒和 HIV-1 感染,在 1 名医护人员(HCW)中存在医院感染。医院为病例管理设立了一个临时隔离病房,成立了一个人类猴痘应对小组,并提供了感染控制资源。在开始时,一些 HCW 不愿意参与疫情应对,而另一些 HCW 则回避疑似患者。一些患者及其家属受到歧视和排斥,也有拒绝隔离的情况。通过所有利益相关者的反复培训和协作,解决了其中的一些挑战,最终成功遏制了疫情。
虽然 2017 年尼日利亚的人类猴痘疫情得到了控制,但我们的报告揭示了疫情应对方面的一些差距,这些差距可以为其他医院提供教训,以加强医院环境中的疫情防范和应对活动。