Baker Heart and Diabetes Institute, Melbourne, VIC, Australia.
Department of Microbiology, Immunology and Tropical Diseases, George Washington University, Washington, DC, United States of America.
PLoS One. 2019 Apr 18;14(4):e0215620. doi: 10.1371/journal.pone.0215620. eCollection 2019.
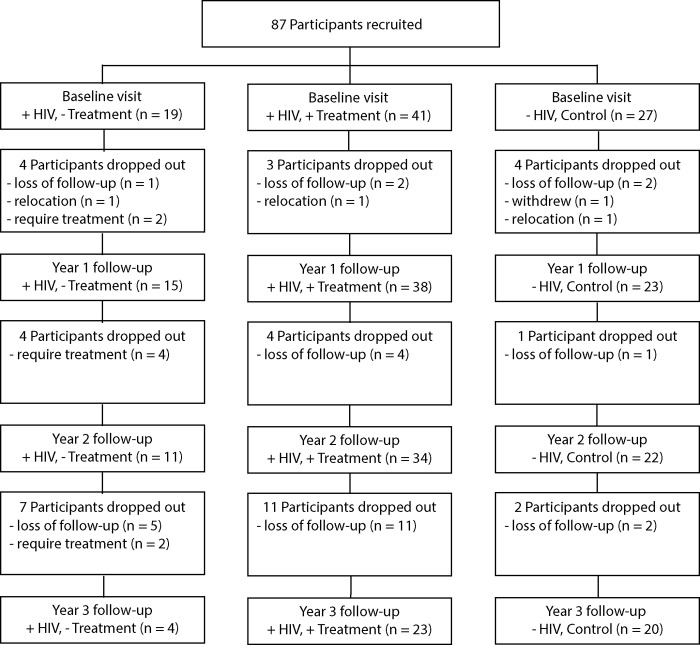
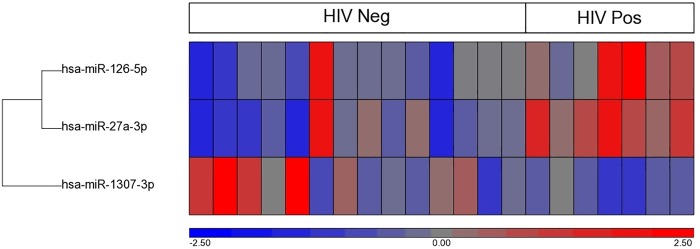
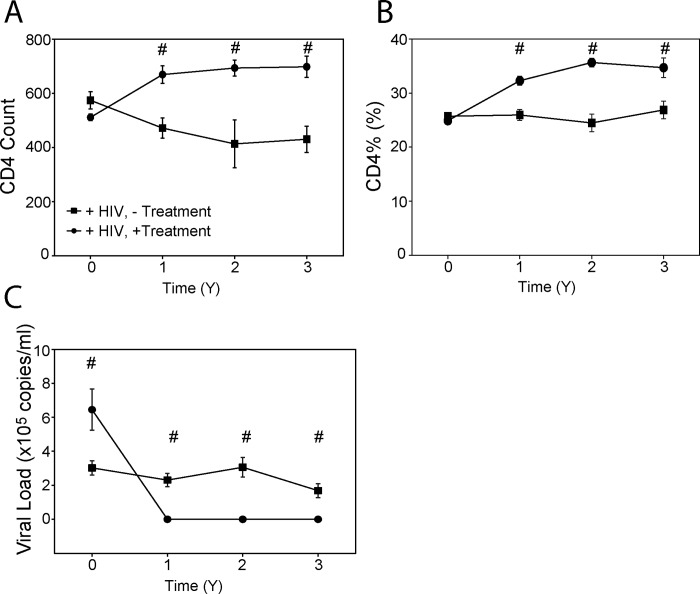
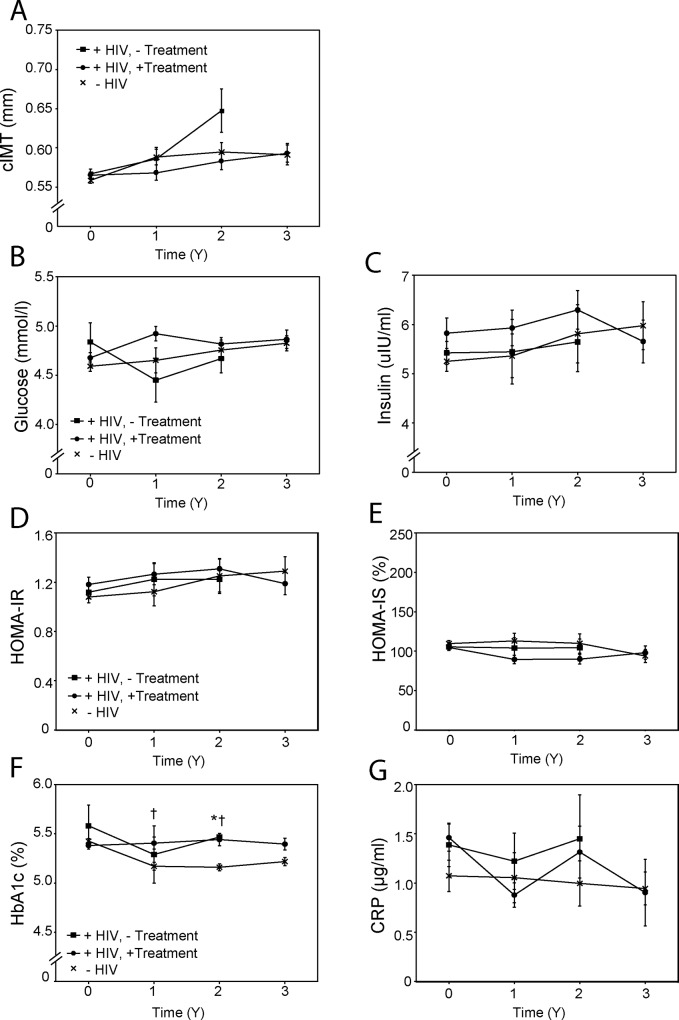
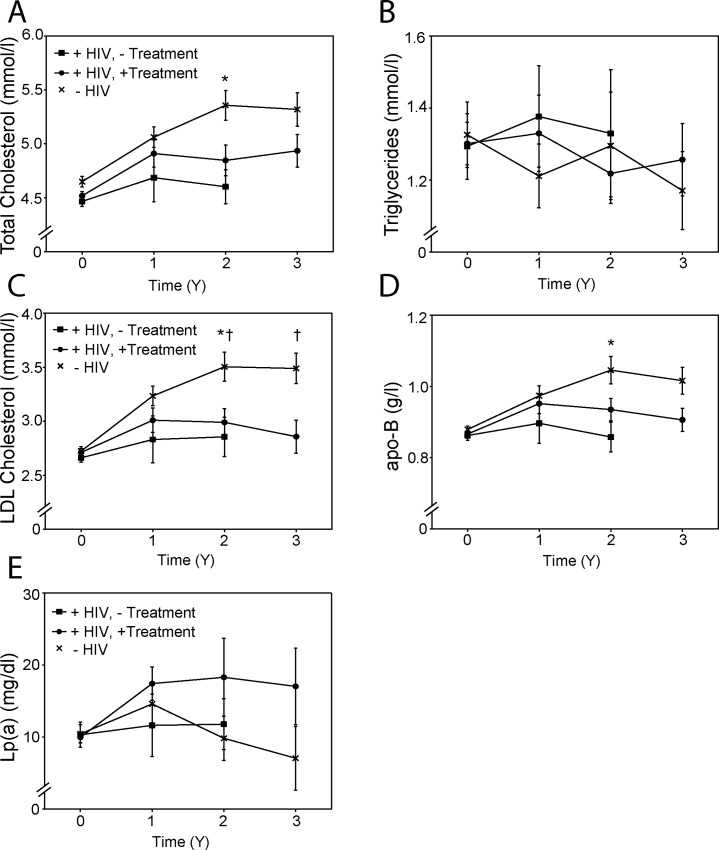
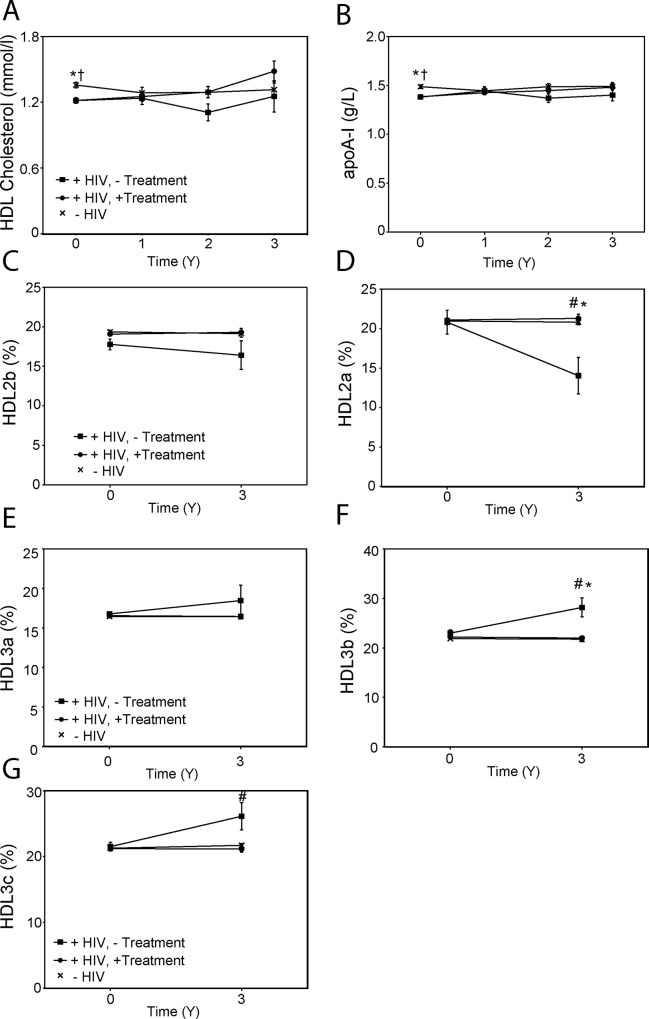
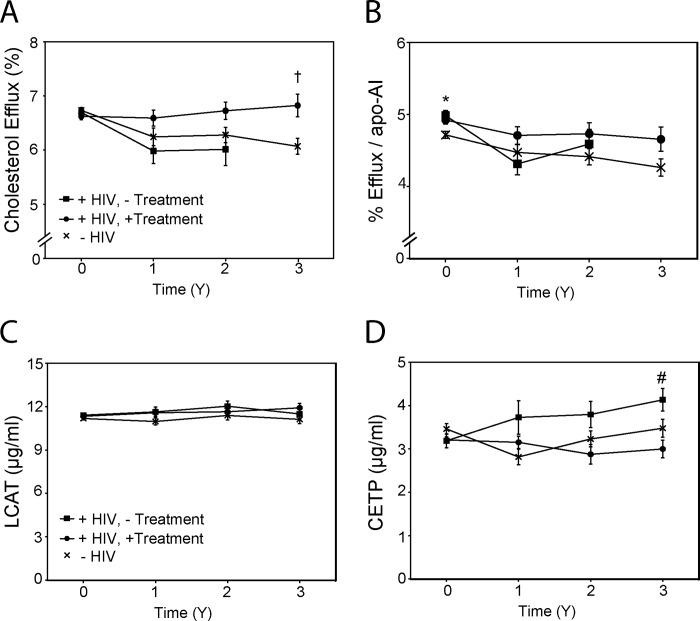
HIV infection is known to be associated with cardiometabolic abnormalities; here we investigated the progression and causes of these abnormalities. Three groups of participants were recruited: HIV-negative subjects and two groups of treatment-naïve HIV-positive subjects, one group initiating antiretroviral treatment, the other remaining untreated. Intima-media thickness (cIMT) increased in HIV-positive untreated group compared to HIV-negative group, but treatment mitigated the difference. We found no increase in diabetes-related metabolic markers or in the level of inflammation in any of the groups. Total cholesterol, low density lipoprotein cholesterol and apoB levels were lower in HIV-positive groups, while triglyceride and Lp(a) levels did not differ between the groups. We found a statistically significant negative association between viral load and plasma levels of total cholesterol, LDL cholesterol, HDL cholesterol, apoA-I and apoB. HIV-positive patients had hypoalphalipoproteinemia at baseline, and we found a redistribution of sub-populations of high density lipoprotein (HDL) particles with increased proportion of smaller HDL in HIV-positive untreated patients, which may result from increased levels of plasma cholesteryl ester transfer protein in this group. HDL functionality declined in the HIV-negative and HIV-positive untreated groups, but not in HIV-positive treated group. We also found differences between HIV-positive and negative groups in plasma abundance of several microRNAs involved in lipid metabolism. Our data support a hypothesis that cardiometabolic abnormalities in HIV infection are caused by HIV and that antiretroviral treatment itself does not influence key cardiometabolic parameters, but mitigates those affected by HIV.
HIV 感染与心血管代谢异常有关;在这里,我们研究了这些异常的进展和原因。我们招募了三组参与者:HIV 阴性受试者和两组未经治疗的 HIV 阳性受试者,一组开始接受抗逆转录病毒治疗,另一组未接受治疗。与 HIV 阴性组相比,未经治疗的 HIV 阳性组的内-中膜厚度(cIMT)增加,但治疗减轻了这种差异。我们没有发现任何一组的糖尿病相关代谢标志物或炎症水平增加。在 HIV 阳性组中,总胆固醇、低密度脂蛋白胆固醇和载脂蛋白 B 水平较低,而甘油三酯和 Lp(a)水平在各组之间没有差异。我们发现病毒载量与总胆固醇、LDL 胆固醇、HDL 胆固醇、载脂蛋白 A-I 和载脂蛋白 B 的血浆水平之间存在统计学上显著的负相关。HIV 阳性患者在基线时有低α脂蛋白血症,我们发现 HIV 未经治疗的患者中高密度脂蛋白(HDL)颗粒的亚群分布发生了重新分布,小 HDL 的比例增加,这可能是由于该组中血浆胆固醇酯转移蛋白水平增加所致。在 HIV 阴性和 HIV 未经治疗的患者组中,HDL 功能下降,但在 HIV 经治疗的患者组中没有下降。我们还发现 HIV 阳性和阴性组之间几种参与脂质代谢的 microRNA 的血浆丰度存在差异。我们的数据支持这样一种假设,即 HIV 感染中的心血管代谢异常是由 HIV 引起的,抗逆转录病毒治疗本身不会影响关键的心血管代谢参数,但可以减轻 HIV 影响的参数。