Davis Josemine, Sreevastava Deepak Kumar, Dwivedi Deepak, Gadgi Siddaramesh, Sud Saurabh, Dudeja Puja
Department of Anesthesia and Critical Care, Command Hospital (Southern Command), Pune, Maharashtra, India.
Department of Community Medicine, Armed Forces Medical College, Pune, Maharashtra, India.
Anesth Essays Res. 2019 Jan-Mar;13(1):13-18. doi: 10.4103/aer.AER_9_19.
Complex gastrointestinal (GI) endoscopic procedures like endoscopic retrograde cholangiopancreatography (ERCP) require deep sedation or general anesthesia. Comorbidities with the poor physiological condition warrant endotracheal intubation to prevent hypoxia and aspiration. The gastro-laryngeal tube (GLT), a new supraglottic airway device with a separate channel for endoscope looks promising.
The aim of the study is to compare the stress response during insertion of GLT and endotracheal intubation (ETT) in patients undergoing upper GI endoscopic procedures like ERCP.
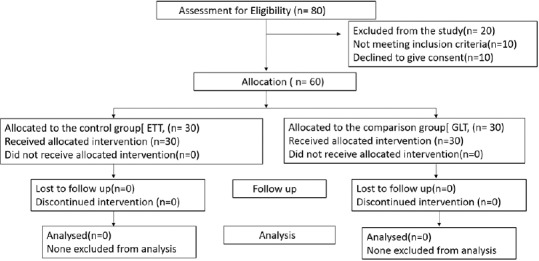
This control versus comparison study comprised two groups with 30 patients each who underwent ETT and GLT insertion. The standard general anesthesia technique was used. In GLT group, the device was inserted without neuromuscular blocker. In ETT group, injection atracurium 0.5 mg/kg intravenous was administered as muscle relaxant for aiding endotracheal intubation. Hemodynamic parameters and time taken for the insertion of GLT/ETT were recorded.
Data were analyzed using SPSS version 20. Student's -test was used to compare quantitative data between the groups. ANOVA test was applied for intragroup comparisons between GLT and ETT groups. Categorical variables were analyzed using the Chi-square test.
Heart rate and mean arterial pressure increased from baseline in ETT group, following laryngoscopy and endotracheal intubation as well as with GLT insertion. However, the stress response caused by endotracheal intubation was significantly greater than that caused by GLT insertion.
GLT as an airway device is a safe alternative with decreased stress response compared to endotracheal intubation for upper GI endoscopy procedures.
诸如内镜逆行胰胆管造影术(ERCP)等复杂的胃肠道(GI)内镜手术需要深度镇静或全身麻醉。生理状况较差的合并症患者需要气管插管以预防缺氧和误吸。胃喉管(GLT)是一种新型声门上气道装置,有一个用于内镜的独立通道,看起来很有前景。
本研究的目的是比较在接受ERCP等上消化道内镜手术的患者中插入GLT和气管插管(ETT)期间的应激反应。
这项对照与比较研究包括两组,每组30例接受ETT和GLT插入的患者。采用标准的全身麻醉技术。在GLT组中,在不使用神经肌肉阻滞剂的情况下插入该装置。在ETT组中,静脉注射0.5mg/kg阿曲库铵作为肌肉松弛剂以辅助气管插管。记录血流动力学参数以及插入GLT/ETT所需的时间。
使用SPSS 20版软件分析数据。采用学生t检验比较两组之间的定量数据。对GLT组和ETT组进行组内比较时应用方差分析。使用卡方检验分析分类变量。
在ETT组中,喉镜检查和气管插管以及插入GLT后,心率和平均动脉压均较基线升高。然而,气管插管引起的应激反应明显大于GLT插入引起的应激反应。
对于上消化道内镜手术,GLT作为一种气道装置是一种安全的选择,与气管插管相比,其应激反应较小。