Division of Hematology, Department of Medicine, Mayo Clinic, Rochester, MN, United States.
Department of Hematology, University of Arizona, Tucson, AZ, United States.
Front Immunol. 2019 Apr 16;10:777. doi: 10.3389/fimmu.2019.00777. eCollection 2019.
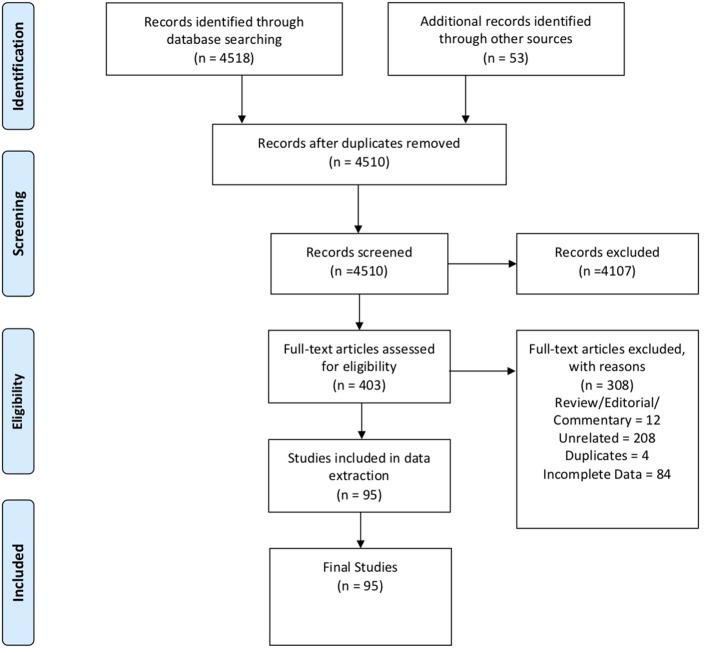
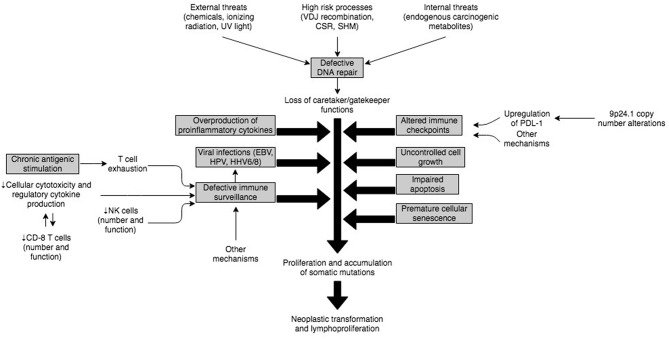
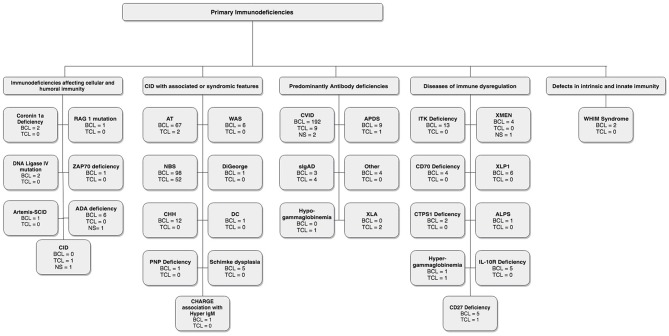
Primary immunodeficiencies and immune dysregulatory disorders (PIDDs; now referred to as inborn errors in immunity) are rare disorders with a prevalence of 41. 4 or 50.5 per 100,000 persons (1). The incidence of malignancy in PIDD patents is the second-highest cause of death in children as well as adults, after infection, and is higher in certain PIDDs compared to others. We performed a systematic review of the literature to identify reports of B cell and T cell neoplasias in PIDDs and clustered them based on their classification in the IUIS schema. As would be expected, higher susceptibility to malignancies are typically reported in patients with Common Variable Immunodeficiency (CVID), combined immunodeficiencies affecting cellular immunity, in particular, DNA repair defects, or in the context of impaired immune regulatory control. There is not much evidence of increased risk for cancer in patients with innate immune defects, indicating that not all types of infection or genetic susceptibility predispose equally to cancer risk. Viral infections, in particular EBV, HHV and HPV, have been shown to increase susceptibility to developing cancer, but also patients with defects in immune regulation, such as Autoimmune Lymphoproliferative Syndrome (ALPS), activated p110delta syndrome (APDS type 1) and IL-10 receptor deficiency among others have a higher incidence of neoplastic disease, particularly lymphomas. In fact, lymphomas account for two-thirds of all malignancies reported in PIDD patients (2), with either a combined immunodeficiency or DNA repair defect predominating as the underlying immune defect in one registry, or antibody deficiencies in another (3). The vast majority of lymphomas reported in the context of PIDDs are B cell lymphomas, though T cell lymphomas have been reported in a few studies, and tend to largely be associated with chromosomal breakage disorders (4) or Cartilage Hair Hypoplasia (5). There appears to be a much higher prevalence of T cell lymphomas in patients with secondary immunodeficiencies (6), though this could reflect treatment bias. We reviewed the literature and summarized the reports of B and T cell lymphoma in PIDD patients to survey the current state of knowledge in this area.
原发性免疫缺陷和免疫调节紊乱(PIDDs;现在称为先天性免疫缺陷)是罕见疾病,患病率为每 10 万人中有 41.4 或 50.5 人(1)。在儿童和成人中,恶性肿瘤是仅次于感染的第二大死亡原因,在某些 PIDDs 中比其他疾病更高。我们对文献进行了系统回顾,以确定 PIDDs 中 B 细胞和 T 细胞肿瘤的报告,并根据它们在 IUIS 方案中的分类进行聚类。正如预期的那样,通常在患有普通可变免疫缺陷(CVID)、影响细胞免疫的联合免疫缺陷、特别是 DNA 修复缺陷的患者中,或在免疫调节控制受损的情况下,报告的恶性肿瘤易感性更高。在具有固有免疫缺陷的患者中,癌症风险增加的证据并不多,这表明并非所有类型的感染或遗传易感性都会同等地增加癌症风险。病毒感染,特别是 EBV、HHV 和 HPV,已被证明会增加发生癌症的易感性,但具有免疫调节缺陷的患者,如自身免疫性淋巴增生综合征(ALPS)、激活的 p110delta 综合征(APDS 型 1)和 IL-10 受体缺陷等,也会有更高的肿瘤疾病发病率,特别是淋巴瘤。事实上,淋巴瘤占 PIDD 患者报告的所有恶性肿瘤的三分之二(2),在一个登记处中,以联合免疫缺陷或 DNA 修复缺陷为主导的免疫缺陷,或在另一个登记处中以抗体缺陷为主导的免疫缺陷(3)。在 PIDDs 背景下报告的绝大多数淋巴瘤是 B 细胞淋巴瘤,尽管在少数研究中报告了 T 细胞淋巴瘤,但它们往往主要与染色体断裂障碍(4)或软骨毛发发育不良(5)相关。在继发性免疫缺陷患者中,T 细胞淋巴瘤的患病率似乎要高得多(6),尽管这可能反映了治疗偏见。我们回顾了文献,并总结了 PIDD 患者中 B 和 T 细胞淋巴瘤的报告,以调查该领域的现有知识状况。