Division of Hematology/Oncology, Department of Medicine, University of Pittsburgh, UPMC Hillman Cancer Center, Pittsburgh, Pennsylvania.
Department of Biostatistics and Computational Biology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts.
Cancer. 2019 Sep 1;125(17):3013-3024. doi: 10.1002/cncr.32162. Epub 2019 May 8.
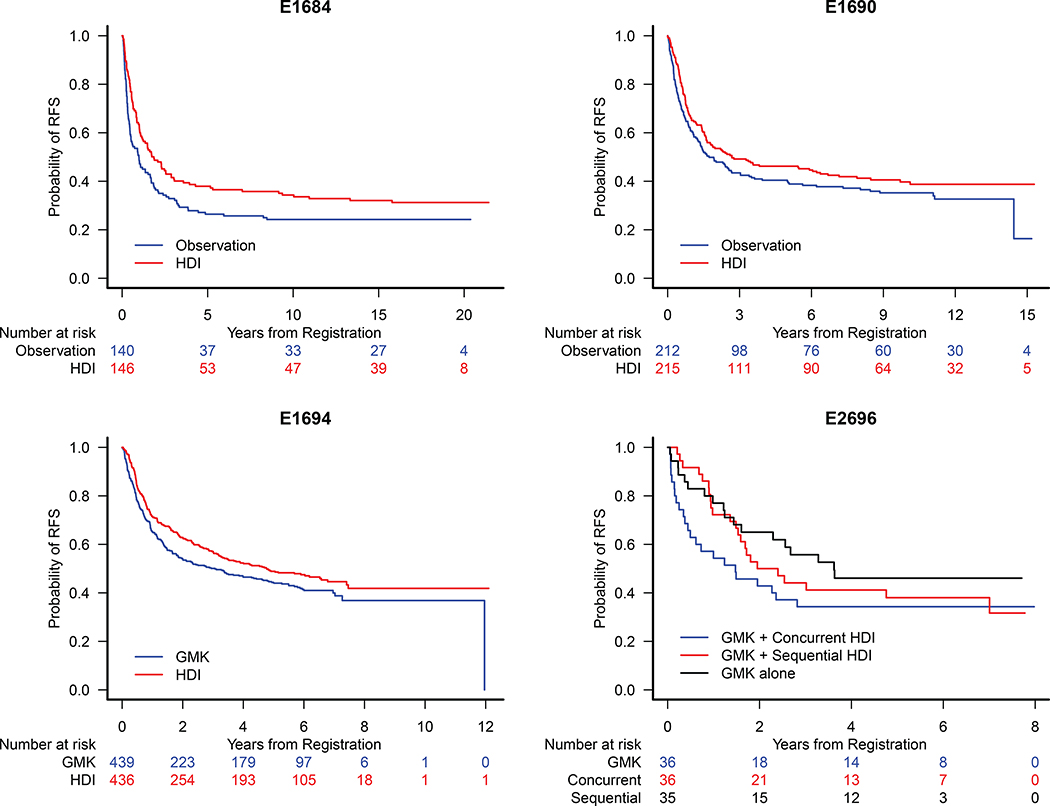
The pivotal E1684, E1690, E1694, and E2696 trials of adjuvant high-dose interferon-α (HDI) enrolled nearly 2000 patients, and established HDI as the standard of care in adjuvant therapy for patients with resected high-risk melanoma. Herein, the authors present an updated analysis of these 4 trials.
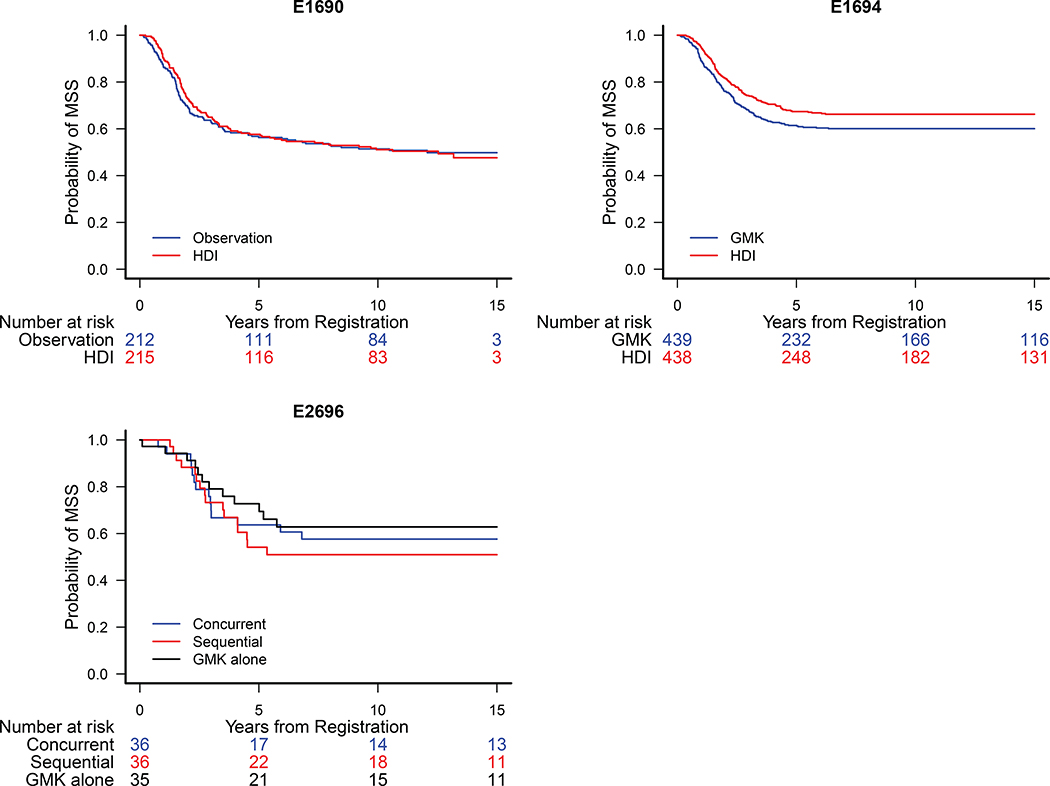
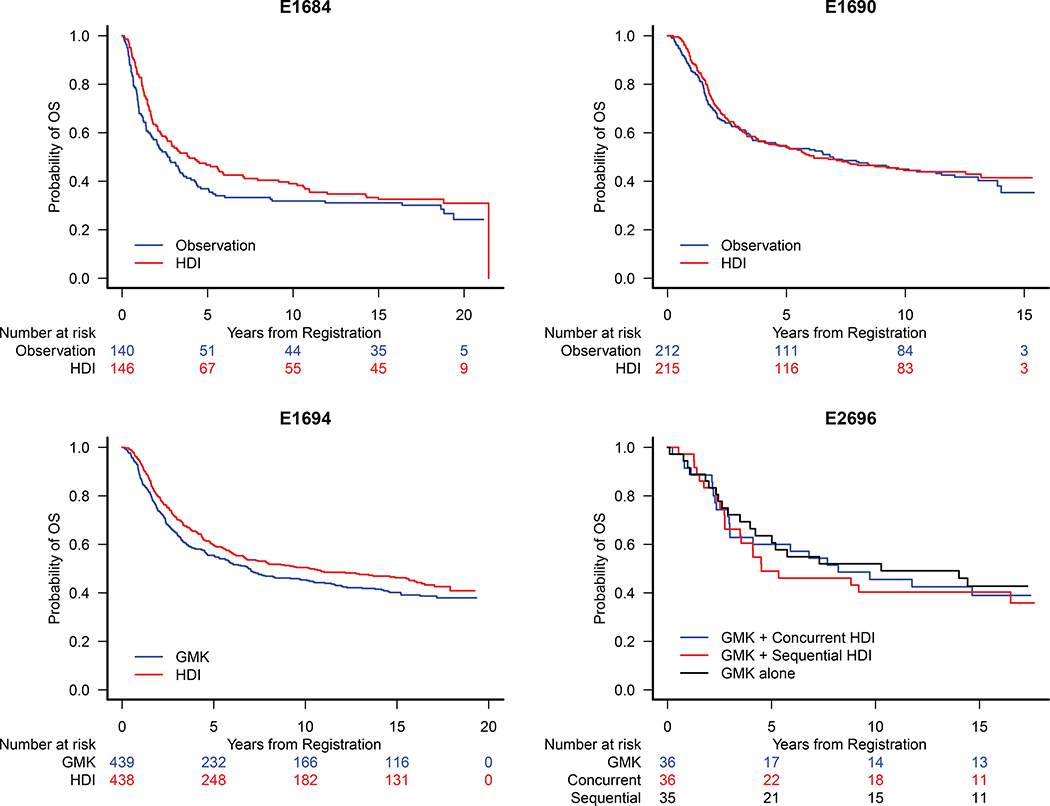
Survival and disease status were updated in September 2016. These data represent a median follow-up of 17.9 years for the E1684 trial, 12.2 years for the E1690 trial, 16.0 years for the E1694 trial, and 16.5 years for the E2696 trial.
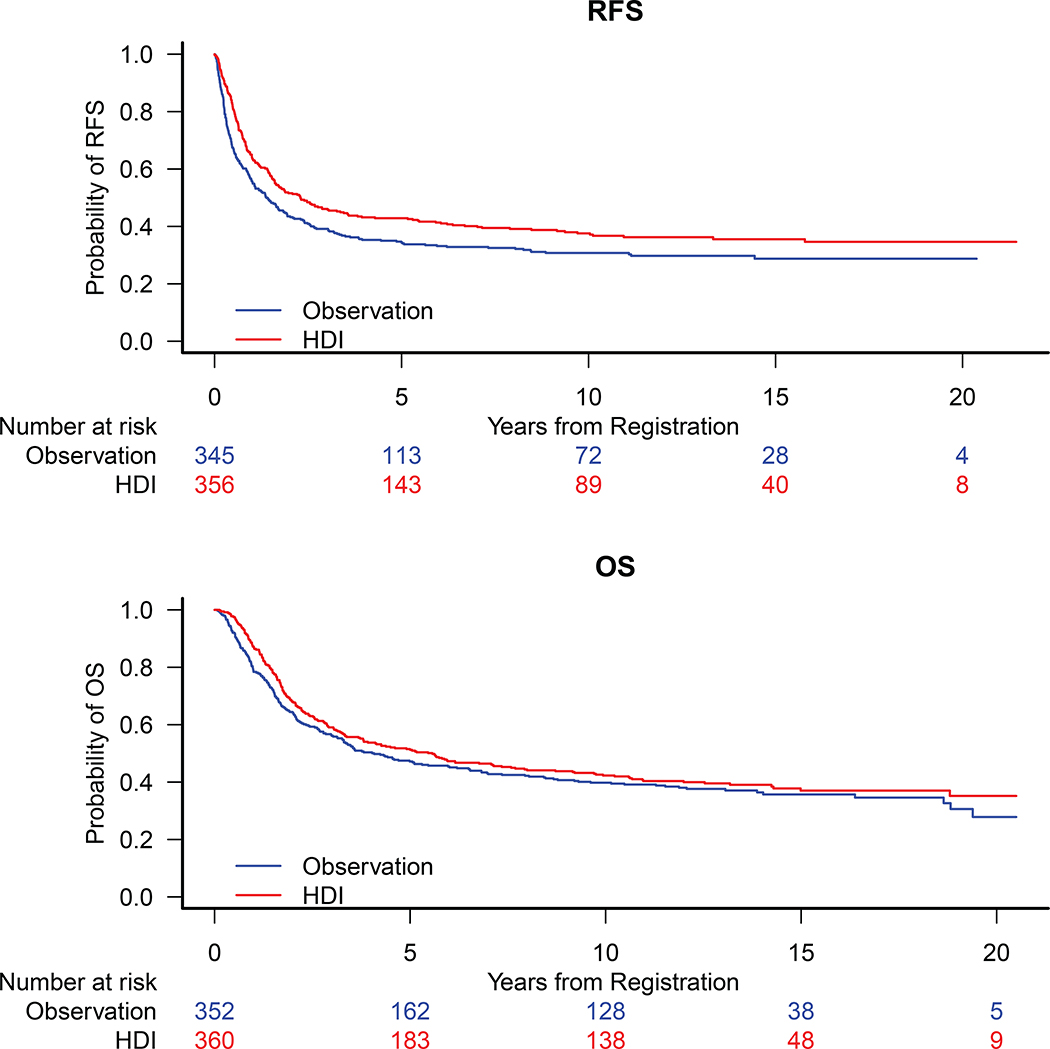
The current analysis confirmed the benefit to recurrence-free survival (RFS) of HDI in the E1684 trial at a median follow-up of 17.9 years. The RFS benefit in the E1694 trial remained evident at a median follow-up of 16 years. Furthermore, the results of the current study confirmed the RFS benefit of adjuvant HDI compared with observation in a pooled analysis of the E1684 and E1690 trials. No overall survival benefit was apparent in this pooled analysis. Updated results for the E1690 and E2696 trials did not differ from those previously reported. In addition, to the authors' knowledge, the current study is the first to report a significant difference in melanoma-specific survival (MSS) between patients treated with HDI compared with the ganglioside GM2/keyhole limpet hemocyanin (GMK) vaccine in the E1694 trial.
In patients with resected high-risk melanoma, adjuvant HDI demonstrated improved RFS in the E1684 and E1694 trials, and improved MSS in a pooled analysis of HDI in the E1694 trial. To the authors' knowledge, these findings represent the most mature level of evidence for the benefit of HDI with respect to RFS and MSS. HDI is the only approved adjuvant treatment for which there are data available in patients with resected stage IIB/IIC melanoma, and remains a reasonable treatment option in this population.
辅助高剂量干扰素-α(HDI)的关键性 E1684、E1690、E1694 和 E2696 试验纳入了近 2000 名患者,确立了 HDI 作为辅助治疗高危黑色素瘤患者的标准治疗方法。在此,作者报告了这 4 项试验的最新分析结果。
生存和疾病状态于 2016 年 9 月进行了更新。这些数据代表 E1684 试验中位随访 17.9 年、E1690 试验中位随访 12.2 年、E1694 试验中位随访 16.0 年和 E2696 试验中位随访 16.5 年的最新分析结果。
当前分析在中位随访 17.9 年时证实了 HDI 对 E1684 试验无复发生存率(RFS)的获益。在中位随访 16 年时,E1694 试验的 RFS 获益仍然明显。此外,当前研究的结果在 E1684 和 E1690 试验的联合分析中证实了辅助 HDI 与观察相比的 RFS 获益。在该联合分析中,未观察到总体生存获益。E1690 和 E2696 试验的更新结果与之前报告的结果没有差异。此外,据作者所知,当前研究首次报道了 E1694 试验中与神经节苷脂 GM2/钥孔血蓝蛋白(GMK)疫苗相比,接受 HDI 治疗的患者在黑色素瘤特异性生存(MSS)方面存在显著差异。
在接受高风险黑色素瘤切除的患者中,E1684 和 E1694 试验中辅助 HDI 显示出 RFS 改善,E1694 试验的联合分析中 HDI 显示出 MSS 改善。据作者所知,这些发现代表了关于 HDI 在 RFS 和 MSS 方面获益的最成熟的证据水平。HDI 是唯一一种在接受 IIB/IIC 期黑色素瘤切除的患者中具有可用数据的辅助治疗方法,并且在该人群中仍然是一种合理的治疗选择。