Department of Obstetrics and Gynecology, University of Helsinki and Helsinki University Hospital, Haartmaninkatu 2, 00029 HUS, Helsinki, Finland.
BMC Pregnancy Childbirth. 2019 May 20;19(1):176. doi: 10.1186/s12884-019-2334-3.
The rates of cesarean section (CS) are increasing worldwide leading to an increased risk for maternal and neonatal complications in the subsequent pregnancy and labor. Previous studies have demonstrated that successful trial of labor after cesarean (TOLAC) is associated with the least maternal morbidity, but the risks of unsuccessful TOLAC exceed the risks of scheduled repeat CS. However, prediction of successful TOLAC is difficult, and only limited data on TOLAC in women with previous failed labor induction or labor dystocia exists. Our aim was to evaluate the success of TOLAC in women with a history of failed labor induction or labor dystocia, to compare the delivery outcomes according to stage of labor at time of previous CS, and to assess the risk factors for recurrent failed labor induction or labor dystocia.
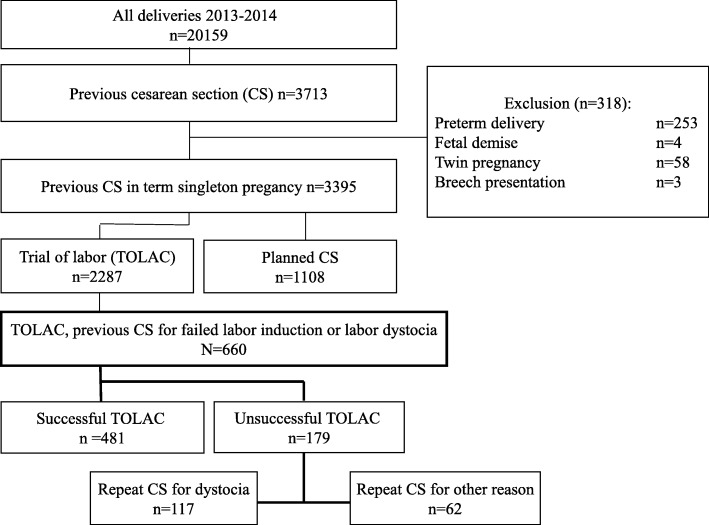
This retrospective cohort study of 660 women with a prior CS for failed labor induction or labor dystocia undergoing TOLAC was carried out in Helsinki University Hospital, Finland, between 2013 and 2015. Data on the study population was obtained from the hospital database and analyzed using SPSS.
The rate of vaginal delivery was 72.9% and the rate of repeat CS for failed induction or labor dystocia was 17.7%. The rate of successful TOLAC was 75.6% in women with a history of labor arrest in the first stage of labor, 73.1% in women with a history of labor arrest in the second stage of labor, and 59.0% in women with previous failed induction. The adjusted risk factors for recurrent failed induction or labor dystocia were maternal height < 160 cm (OR 1.9 95% CI 1.1-3.1), no prior vaginal delivery (OR 8.3 95% CI 3.5-19.8), type 1 or gestational diabetes (OR 1.8 95% CI 1.0-3.0), IOL for suspected non-diabetic fetal macrosomia (OR 10.8 95% CI 2.1-55.9) and birthweight ≥4500 g (OR 3.3 95% CI 1.3-7.9).
TOLAC is a feasible option to scheduled repeat CS in women with a history of failed induction or labor dystocia. However, women with no previous vaginal delivery, maternal height < 160 cm, diabetes or suspected neonatal macrosomia (≥4500 g) may be at increased risk for failed TOLAC.
剖宫产率(CS)在全球范围内呈上升趋势,导致随后妊娠和分娩中产妇和新生儿并发症的风险增加。先前的研究表明,剖宫产术后阴道试产(TOLAC)的成功率与产妇发病率最低有关,但 TOLAC 不成功的风险超过了计划性重复 CS 的风险。然而,TOLAC 成功的预测较为困难,仅有有限的数据涉及既往引产失败或产程延长的 TOLAC。我们的目的是评估有既往引产失败或产程延长史的妇女 TOLAC 的成功率,根据既往 CS 时的产程阶段比较分娩结局,并评估复发性引产失败或产程延长的危险因素。
这项回顾性队列研究纳入了 2013 年至 2015 年期间在芬兰赫尔辛基大学医院接受 TOLAC 的 660 名因引产失败或产程延长而行剖宫产的妇女。研究人群的数据来自医院数据库,并使用 SPSS 进行分析。
阴道分娩率为 72.9%,因引产失败或产程延长而再次行 CS 的比率为 17.7%。在第一产程有产程停滞史的妇女中,TOLAC 成功的比例为 75.6%,第二产程有产程停滞史的妇女中 TOLAC 成功的比例为 73.1%,既往引产失败的妇女中 TOLAC 成功的比例为 59.0%。复发性引产失败或产程延长的调整后危险因素包括:母亲身高<160cm(OR 1.9,95%CI 1.1-3.1)、无既往阴道分娩史(OR 8.3,95%CI 3.5-19.8)、1 型或妊娠期糖尿病(OR 1.8,95%CI 1.0-3.0)、因疑似非糖尿病巨大儿行 IOL(OR 10.8,95%CI 2.1-55.9)和出生体重≥4500g(OR 3.3,95%CI 1.3-7.9)。
TOLAC 是既往引产失败或产程延长的妇女计划性重复 CS 的可行选择。然而,无既往阴道分娩史、母亲身高<160cm、糖尿病或疑似巨大儿(≥4500g)的妇女 TOLAC 失败的风险可能增加。