Hiki Naoki, Nunobe Souya
Department of Upper Gastrointestinal Surgery Kitasato University School of Medicine Sagamihara Kanagawa Japan.
Department of Gastroenterological Surgery Cancer Institute Ariake Hospital Japanese Foundation for Cancer Research Tokyo Japan.
Ann Gastroenterol Surg. 2019 Feb 19;3(3):239-246. doi: 10.1002/ags3.12238. eCollection 2019 May.
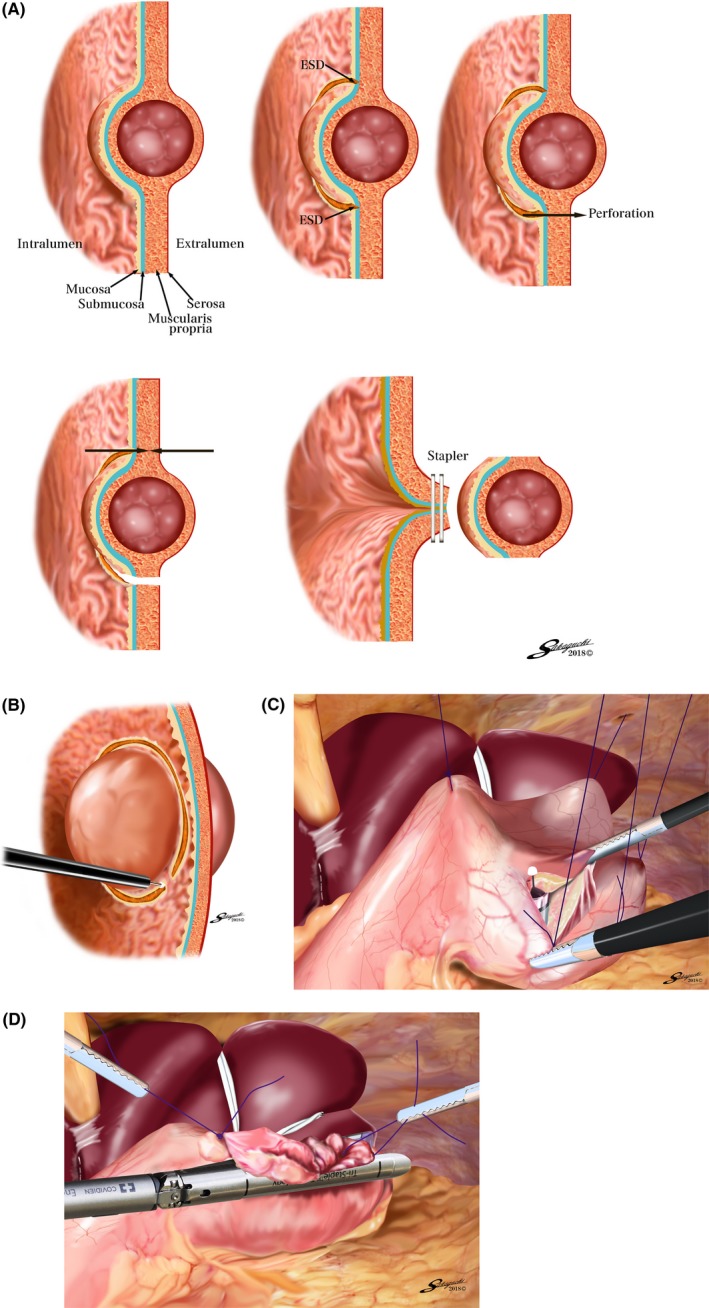
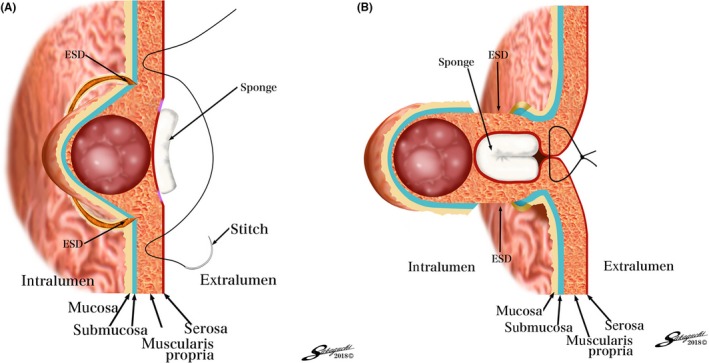
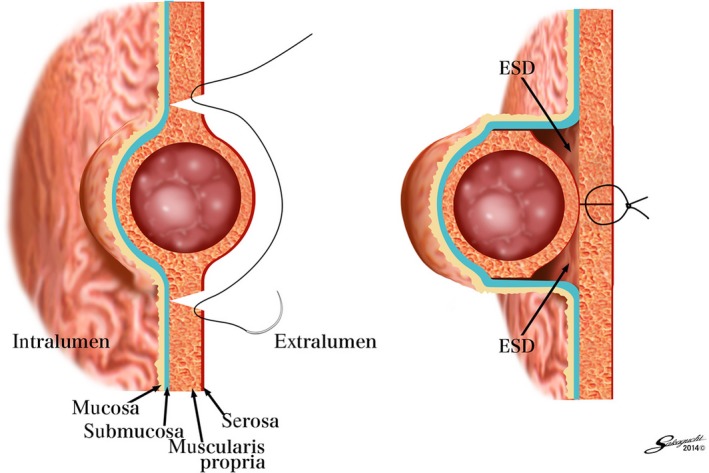
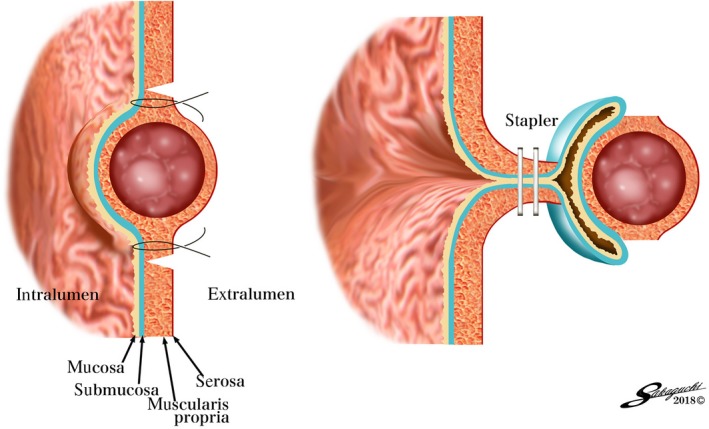
Laparoscopic and endoscopic cooperative surgery (LECS) is a procedure combining laparoscopic gastric resection with endoscopic submucosal dissection for local resection of gastric tumors with appropriate, minimal surgical resection margins. The LECS concept was initially developed from the classical LECS procedure for gastric submucosal tumor resection. Many researchers reported that classical LECS was a safe and feasible technique for resection of gastric submucosal tumors, regardless of tumor location, including the esophagogastric junction. Recently, LECS was approved for insurance coverage by Japan's National Health Insurance plan and widely applied for gastric submucosal tumor resection. However, the limitations of classical LECS are the risk of abdominal infection, scattering of tumor cells in the abdominal cavity, and tumor cell seeding in the peritoneum. The development of modified LECS procedures, such as inverted-LECS, non-exposed endoscopic wall-inversion surgery, a combination of laparoscopic and endoscopic approaches to neoplasia with a non-exposure technique, and closed-LECS, has almost resolved these drawbacks. This has led to a recent increase in the indication of modified LECS to include patients with gastric epithelial neoplasms. The LECS concept is also beginning to be applied to tumor excision in other organs, such as the duodenum, colon and rectum. Further evolution of LECS procedures is expected in the future. Sentinel lymph node mapping could also be combined with LECS, resulting in a portion of early gastric cancers being treated by LECS with sentinel node mapping.
腹腔镜与内镜联合手术(LECS)是一种将腹腔镜胃切除术与内镜黏膜下剥离术相结合的手术方法,用于对胃肿瘤进行局部切除,并确保手术切缘适当且最小。LECS概念最初源于用于胃黏膜下肿瘤切除的经典LECS手术。许多研究人员报告称,经典LECS是一种安全可行的胃黏膜下肿瘤切除技术,无论肿瘤位于何处,包括食管胃交界部。最近,LECS被日本国民健康保险计划批准纳入保险范围,并广泛应用于胃黏膜下肿瘤切除。然而,经典LECS的局限性在于存在腹部感染风险、肿瘤细胞在腹腔内播散以及肿瘤细胞种植于腹膜的风险。改良LECS手术的发展,如倒置LECS、非暴露内镜壁翻转手术、腹腔镜与内镜联合肿瘤切除非暴露技术以及闭合LECS,几乎解决了这些缺点。这导致最近改良LECS的适应证有所增加,包括胃上皮肿瘤患者。LECS概念也开始应用于其他器官的肿瘤切除,如十二指肠、结肠和直肠。预计未来LECS手术将进一步发展。前哨淋巴结 mapping也可与LECS相结合,从而使一部分早期胃癌通过LECS联合前哨淋巴结 mapping进行治疗。