Wills Anne Marie, Garry Jamie, Hubbard Jane, Mezoian Taylor, Breen Christopher T, Ortiz-Miller Courtney, Nalipinski Paige, Sullivan Stacey, Berry James D, Cudkowicz Merit, Paganoni Sabrina, Chan James, Macklin Eric A
Neurology Clinical Research Institute, Department of Neurology, Massachusetts General Hospital, Boston, MA, 02114, USA.
Harvard Medical School, Boston, MA, USA.
BMC Neurol. 2019 May 29;19(1):104. doi: 10.1186/s12883-019-1330-6.
Nutritional status is an important prognostic factor in Amyotrophic Lateral Sclerosis (ALS). We wished to study the safety, tolerability and efficacy of nutritional counseling with or without an mHealth application to maintain or increase body weight in ALS, compared to standard care.
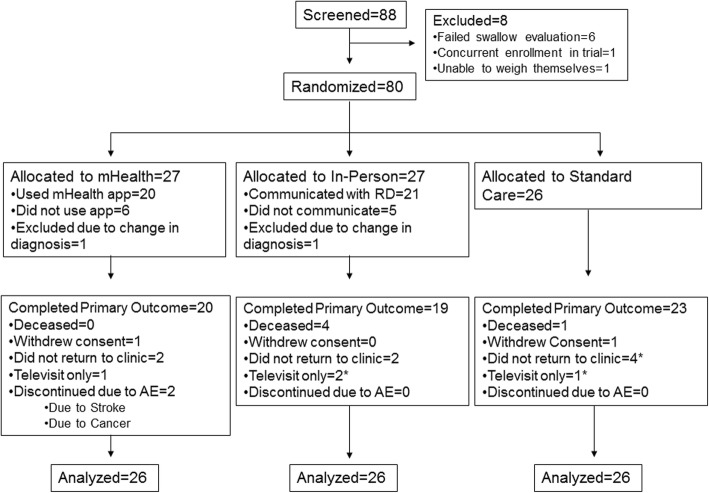
In this randomized open-label, standard-of-care-controlled, single-center clinical trial, we randomly assigned adults with ALS to one of three nutritional interventions: counseling by their physician or nurse ("standard care"), counseling by a registered dietitian (RD) ("in-person"), or counseling supported by a mHealth app ("mHealth"). Both intervention arms received tailored nutrition recommendations and recorded dietary intake and weight biweekly (mHealth) or monthly (in-person). The primary outcome of weight and secondary and tertiary outcomes of calorie intake, ALSFRS-R, and quality of life (QOL) were recorded at each clinic visit and analyzed in an ITT mixed model analysis.
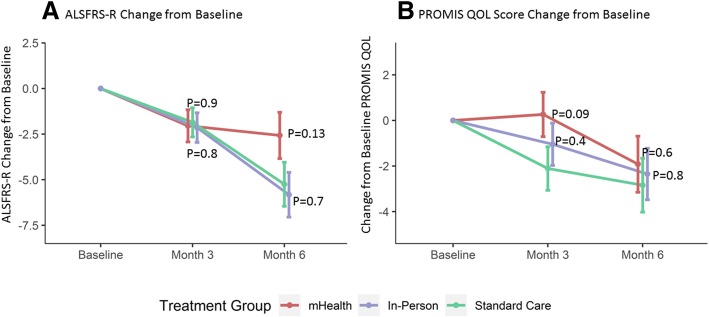
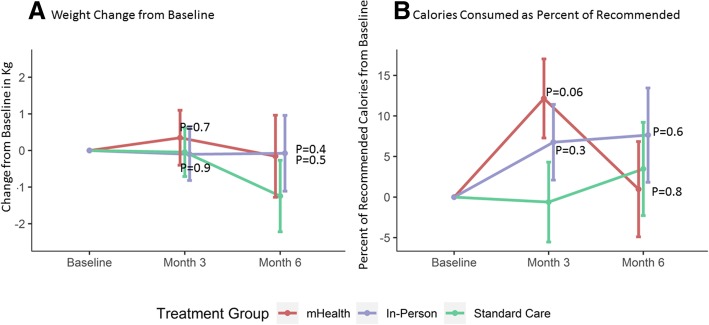
A total of 88 participants were enrolled of whom 78 were included in this analysis. The three arms were well-balanced except for excess males in the mHealth arm and greater weight lost at baseline in the in-person arm. Participants in the mHealth arm increased their calorie intake at month 3 to an average of 94% (95% CI: 85, 103) of recommended calories, compared to 81% (95% CI: 72, 91, p = 0.06 vs. mHealth) in the standard care arm. After 6 months, calorie intake was not different among the three arms. Overall weight was stable across all three groups. QOL scores in the mHealth arm were stable over 3 months (0.3 points, 95% CI: - 1.7, 2.2) compared to worsening in standard care (- 2.1 points, 95% CI: - 4.0, - 0.2, p = 0.09 vs. mHealth), but all scores declined by 6 months. ALSFRS-R total scores declined by an average of - 2.6 points (95% CI: - 5.1, - 0.1) over 6 months in the mHealth arm (p = 0.13 vs. standard care) compared to - 5.8 points (95% CI: - 8.2, - 3.4, p = 0.74 vs. standard care) in the in-person and - 5.2 points (95% CI: - 7.6, - 2.9) in the standard care arm.
Nutritional counseling by a registered dietitian (with or without support by an mHealth app) is safe but did not maintain weight significantly better than standard care in ALS patients.
https://clinicaltrials.gov/ identifier NCT02418546. Registered April 16, 2015.
营养状况是肌萎缩侧索硬化症(ALS)的一个重要预后因素。我们希望研究与标准护理相比,有或没有移动健康(mHealth)应用程序的营养咨询在维持或增加ALS患者体重方面的安全性、耐受性和有效性。
在这项随机开放标签、标准护理对照的单中心临床试验中,我们将成年ALS患者随机分配到三种营养干预措施之一:由其医生或护士进行咨询(“标准护理”)、由注册营养师(RD)进行咨询(“面对面”)或由mHealth应用程序支持的咨询(“mHealth”)。两个干预组都接受了量身定制的营养建议,并每两周(mHealth)或每月(面对面)记录饮食摄入量和体重。每次门诊就诊时记录体重的主要结果以及卡路里摄入量、ALS功能评定量表修订版(ALSFRS-R)和生活质量(QOL)的次要和三级结果,并在意向性分析的混合模型分析中进行分析。
总共招募了88名参与者,其中78名纳入本分析。除了mHealth组男性过多以及面对面组基线时体重下降更多外,三组情况均衡。mHealth组参与者在第3个月时卡路里摄入量增加至推荐卡路里的平均94%(95%CI:85,103),而标准护理组为81%(95%CI:72,91,与mHealth组相比p = 0.06)。6个月后,三组之间的卡路里摄入量没有差异。所有三组的总体体重均保持稳定。mHealth组的QOL评分在3个月内保持稳定(0.3分,95%CI:-1.7,2.2),而标准护理组则恶化(-2.1分,95%CI:-4.0,-0.2,与mHealth组相比p = 0.09),但所有评分在6个月时均下降。mHealth组的ALSFRS-R总分在6个月内平均下降-2.6分(95%CI:-5.1,-0.1)(与标准护理组相比p = 0.13),面对面组为-5.8分(95%CI:-8.2,-3.4,与标准护理组相比p = 0.74),标准护理组为-5.2分(95%CI:-7.6,-2.9)。
由注册营养师进行的营养咨询(无论是否有mHealth应用程序的支持)是安全的,但在ALS患者中,其维持体重的效果并不显著优于标准护理。