Darrah Patricia A, DiFazio Robert M, Maiello Pauline, Gideon Hannah P, Myers Amy J, Rodgers Mark A, Hackney Joshua A, Lindenstrom Thomas, Evans Thomas, Scanga Charles A, Prikhodko Victor, Andersen Peter, Lin Philana Ling, Laddy Dominick, Roederer Mario, Seder Robert A, Flynn JoAnne L
1Vaccine Research Center, National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH), Bethesda, MD USA.
2Department of Microbiology and Molecular Genetics, University of Pittsburgh School of Medicine, Pittsburgh, PA USA.
NPJ Vaccines. 2019 May 28;4:21. doi: 10.1038/s41541-019-0113-9. eCollection 2019.
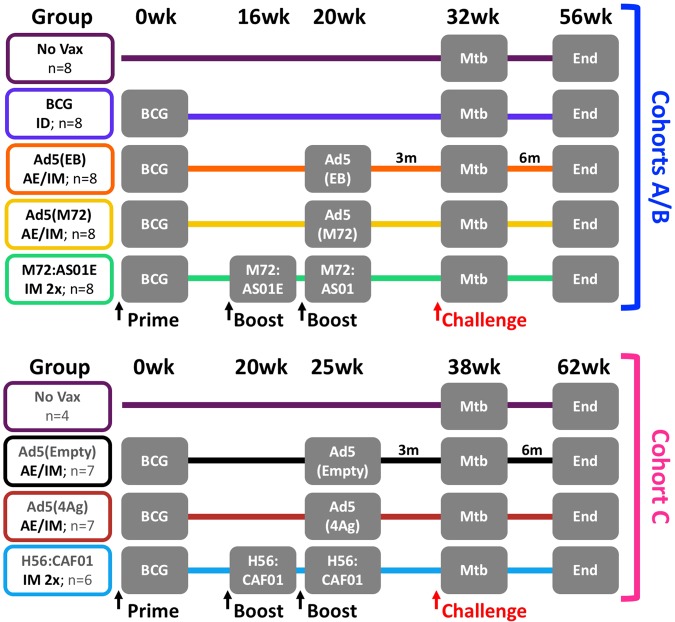
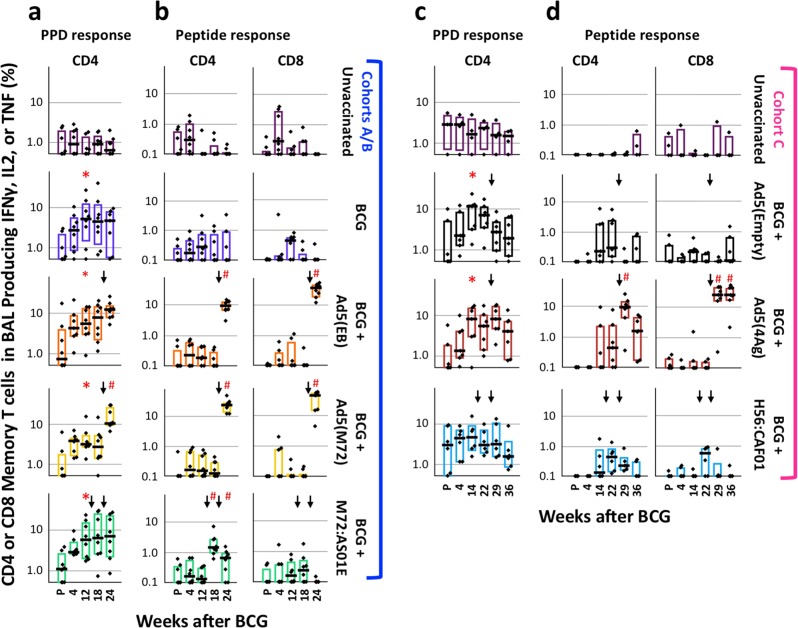
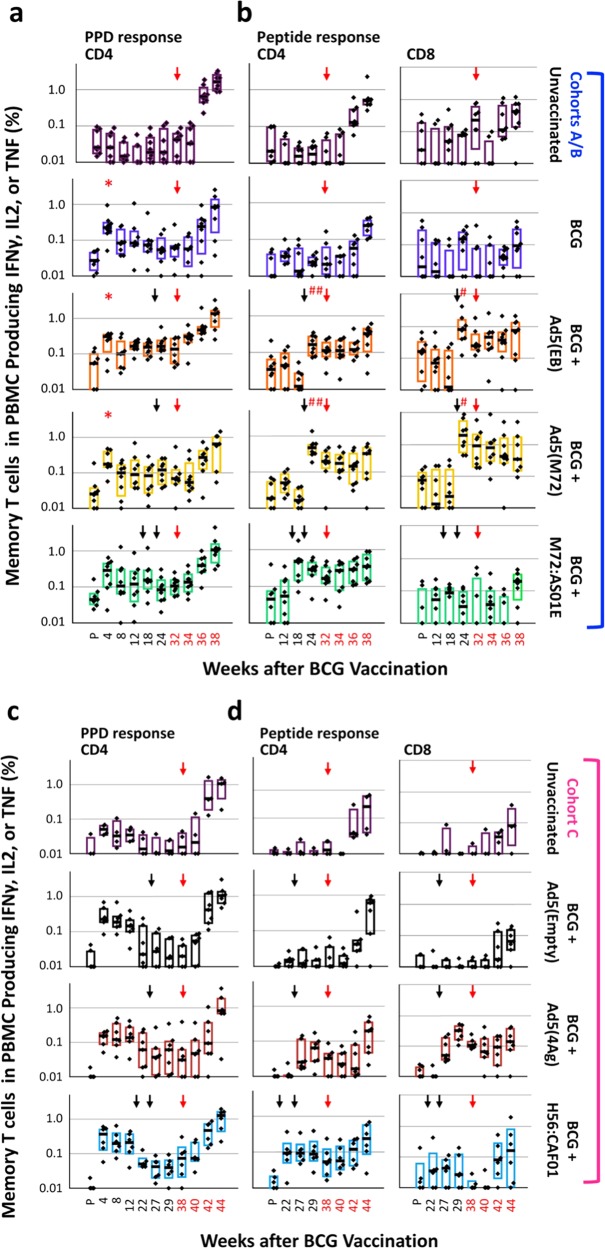
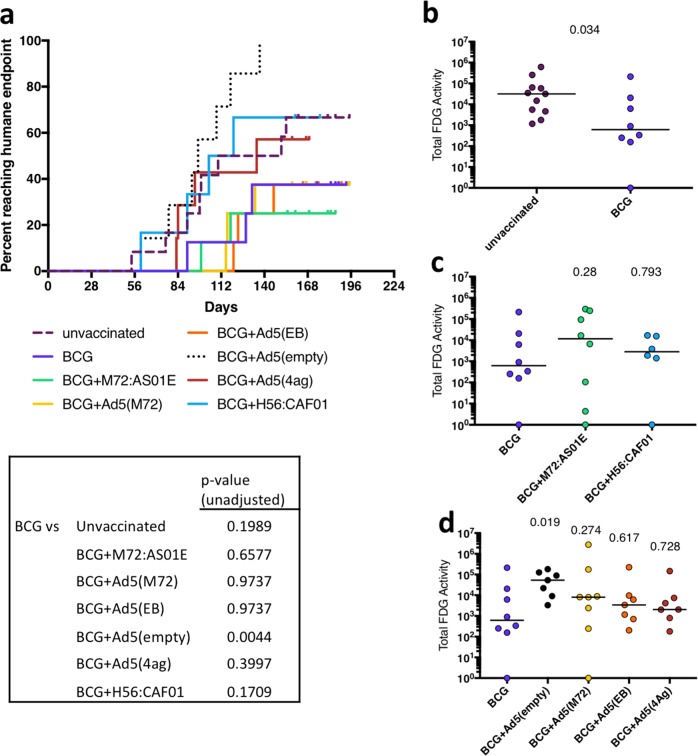
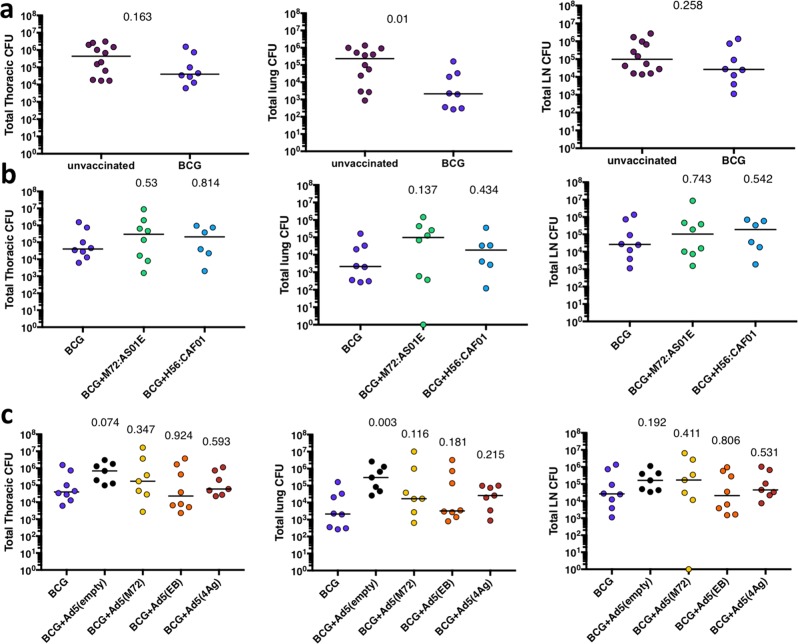
Tuberculosis (TB) is the leading cause of death from infection worldwide. The only approved vaccine, BCG, has variable protective efficacy against pulmonary TB, the transmissible form of the disease. Therefore, improving this efficacy is an urgent priority. This study assessed whether heterologous prime-boost vaccine regimens in which BCG priming is boosted with either (i) protein and adjuvant (M72 plus AS01 or H56 plus CAF01) delivered intramuscularly (IM), or (ii) replication-defective recombinant adenovirus serotype 5 (Ad5) expressing various (Mtb) antigens (Ad5(TB): M72, ESAT-6/Ag85b, or ESAT-6/Rv1733/Rv2626/RpfD) administered simultaneously by IM and aerosol (AE) routes, could enhance blood- and lung-localized T-cell immunity and improve protection in a nonhuman primate (NHP) model of TB infection. Ad5(TB) vaccines administered by AE/IM routes following BCG priming elicited ~10-30% antigen-specific CD4 and CD8 T-cell multifunctional cytokine responses in bronchoalveolar lavage (BAL) but did not provide additional protection compared to BCG alone. Moreover, AE administration of an Ad5(empty) control vector after BCG priming appeared to diminish protection induced by BCG. Boosting BCG by IM immunization of M72/AS01 or H56:CAF01 elicited ~0.1-0.3% antigen-specific CD4 cytokine responses in blood with only a transient increase of ~0.5-1% in BAL; these vaccine regimens also failed to enhance BCG-induced protection. Taken together, this study shows that boosting BCG with protein/adjuvant or Ad-based vaccines using these antigens, by IM or IM/AE routes, respectively, do not enhance protection against primary infection compared with BCG alone, in the highly susceptible rhesus macaque model of tuberculosis.
结核病(TB)是全球感染致死的首要原因。唯一获批的疫苗卡介苗(BCG)对肺结核(该疾病的可传播形式)的保护效力参差不齐。因此,提高其效力是当务之急。本研究评估了以下两种异源初免 - 加强疫苗方案:(i)用肌肉注射(IM)的蛋白质和佐剂(M72加AS01或H56加CAF01)加强卡介苗初免;(ii)通过IM和气溶胶(AE)途径同时接种表达各种结核分枝杆菌(Mtb)抗原的复制缺陷型重组腺病毒5型(Ad5)(Ad5(TB):M72、ESAT - 6/Ag85b或ESAT - 6/Rv1733/Rv2626/RpfD),是否能增强血液和肺局部的T细胞免疫,并在结核病感染的非人灵长类动物(NHP)模型中改善保护效果。在卡介苗初免后通过AE/IM途径接种Ad5(TB)疫苗,在支气管肺泡灌洗(BAL)中引发了约10 - 30%的抗原特异性CD4和CD8 T细胞多功能细胞因子反应,但与单独使用卡介苗相比,并未提供额外的保护。此外,在卡介苗初免后通过AE途径接种Ad5(空载体)对照载体似乎会削弱卡介苗诱导的保护作用。通过IM免疫M72/AS01或H56:CAF01加强卡介苗,在血液中引发了约0.1 - 0.3%的抗原特异性CD4细胞因子反应,在BAL中仅短暂增加了约0.5 - 1%;这些疫苗方案也未能增强卡介苗诱导的保护作用。综上所述,本研究表明,在高度易感的恒河猴结核病模型中,分别通过IM或IM/AE途径,用这些抗原的蛋白质/佐剂或基于Ad的疫苗加强卡介苗,与单独使用卡介苗相比,并未增强对原发性感染的保护作用。