Department of Radiology and Nuclear Medicine, Amsterdam University Medical Centers - location VUmc, De Boelelaan 1117, 1081 HV, Amsterdam, The Netherlands.
Department of Anesthesiology, Amsterdam University Medical Centers - location VUmc, De Boelelaan 1117, 1081 HV, Amsterdam, The Netherlands.
Cardiovasc Intervent Radiol. 2019 Nov;42(11):1597-1608. doi: 10.1007/s00270-019-02273-y. Epub 2019 Jun 26.
In percutaneous ablation procedures, periprocedural pain, unrest and respiratory concerns can be detrimental to achieve a safe and efficacious ablation and impair treatment outcome. This study aimed to compare the association between anesthetic technique and local disease control in patients undergoing percutaneous microwave ablation (MWA) of colorectal liver metastases (CRLM) and hepatocellular carcinoma (HCC).
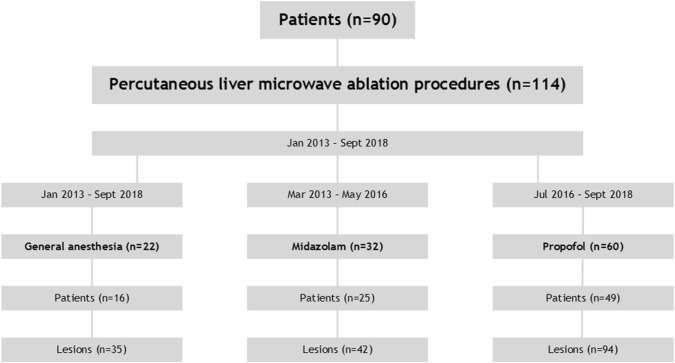
This IRB-exempted single-center comparative, retrospective analysis of three cohorts analyzed 90 patients treated for hepatic malignancies from January 2013 until September 2018. The local tumor progression-free survival (LTPFS), safety and periprocedural pain perception were assessed using univariate and multivariate Cox proportional hazard regression analyses to correct for potential confounders.
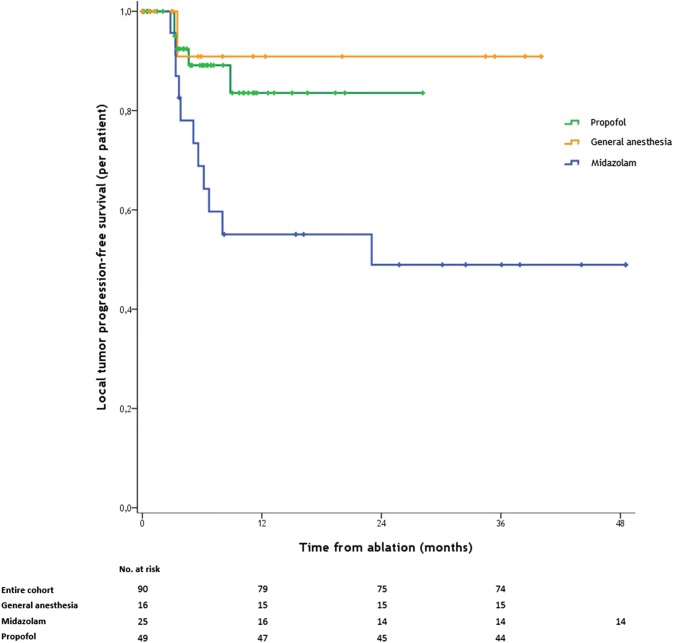
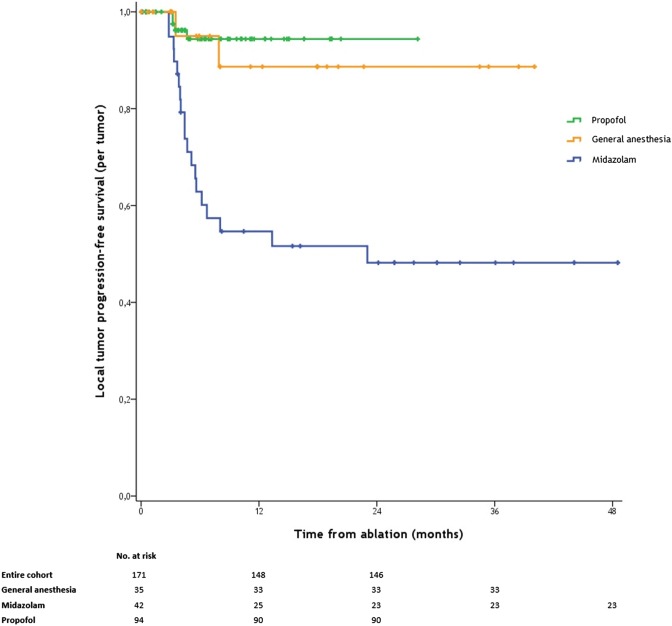
In 114 procedures (22 general anesthesia; 32 midazolam; 60 propofol), 171 liver tumors (136 CRLM; 35 HCC) were treated with percutaneous MWA. Propofol and general anesthesia were superior to midazolam/fentanyl sedation regarding LTPFS (4/94 [4.3%] vs. 19/42 [45.2%] vs. 2/35 [5.7%]; P < 0.001, respectively). Local tumor progression rate was 14.6% (25/171). Eighteen tumors (72.0%) were retreated by ablation. Of them, 14 (78%) were previously treated with midazolam. Propofol versus midazolam (P < 0.001), general anesthesia versus midazolam (P = 0.016), direct postprocedural visual analog pain score above 5 (P = 0.050) and more than one tumor per procedure (P = 0.045) were predictors for LTPFS. Multivariate analysis revealed that propofol versus midazolam (HR 7.94 [95% CI 0.04-0.39; P < 0.001]) and general anesthesia versus midazolam (HR 6.33 [95% CI 0.04-0.69; P = 0.014]) were associated with LTPFS. Pain during and directly after treatment was significantly worse in patients who received midazolam sedation (P < 0.001).
Compared to propofol and general anesthesia, midazolam/fentanyl sedation was associated with an increased periprocedural perception of pain and lower local tumor progression-free survival. To reduce the number of repeat procedures required to eradicate hepatic malignancies, general anesthesia and propofol sedation should be favored over midazolam.
在经皮消融手术中,围手术期疼痛、不安和呼吸问题可能会对安全有效的消融造成不利影响,并影响治疗效果。本研究旨在比较麻醉技术与经皮微波消融(MWA)治疗结直肠癌肝转移(CRLM)和肝细胞癌(HCC)患者局部疾病控制的相关性。
本研究为回顾性、单中心、对照研究,分析了 2013 年 1 月至 2018 年 9 月期间接受肝恶性肿瘤治疗的 90 例患者,共 114 例(22 例全身麻醉;32 例咪达唑仑;60 例丙泊酚)。使用单变量和多变量 Cox 比例风险回归分析评估局部肿瘤无进展生存期(LTPFS)、安全性和围手术期疼痛感知,以纠正潜在的混杂因素。
在 171 个肝脏肿瘤(136 个 CRLM;35 个 HCC)中,有 114 个接受了经皮 MWA 治疗。与咪达唑仑/芬太尼镇静相比,丙泊酚和全身麻醉在 LTPFS 方面更优(4/94[4.3%] vs. 19/42[45.2%] vs. 2/35[5.7%];P<0.001)。局部肿瘤进展率为 14.6%(25/171)。18 个肿瘤(72.0%)接受了消融治疗。其中,14 个(78%)之前接受过咪达唑仑治疗。丙泊酚与咪达唑仑(P<0.001)、全身麻醉与咪达唑仑(P=0.016)、术后即刻视觉模拟疼痛评分>5 分(P=0.050)和每个手术超过一个肿瘤(P=0.045)是 LTPFS 的预测因素。多变量分析显示,与咪达唑仑相比,丙泊酚(HR 7.94[95%CI 0.04-0.39;P<0.001])和全身麻醉(HR 6.33[95%CI 0.04-0.69;P=0.014])与 LTPFS 相关。接受咪达唑仑镇静的患者在治疗期间和治疗后直接感到疼痛明显更严重(P<0.001)。
与丙泊酚和全身麻醉相比,咪达唑仑/芬太尼镇静与围手术期疼痛感知增加和局部肿瘤无进展生存期降低相关。为了减少根除肝恶性肿瘤所需的重复治疗次数,应优先选择全身麻醉和丙泊酚镇静,而不是咪达唑仑。