Myeloma Unit, Division of Hematology, University of Torino, Azienda-Ospedaliero Universitaria (AOU) Città della Salute e della Scienza di Torino, Torino, Italy
Myeloma Unit, Division of Hematology, University of Torino, Azienda-Ospedaliero Universitaria (AOU) Città della Salute e della Scienza di Torino, Torino, Italy.
Haematologica. 2020 Apr;105(4):1074-1080. doi: 10.3324/haematol.2019.220657. Epub 2019 Jun 27.
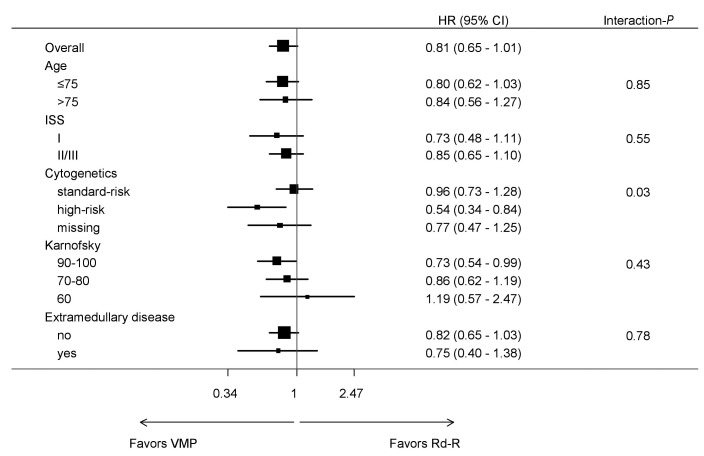
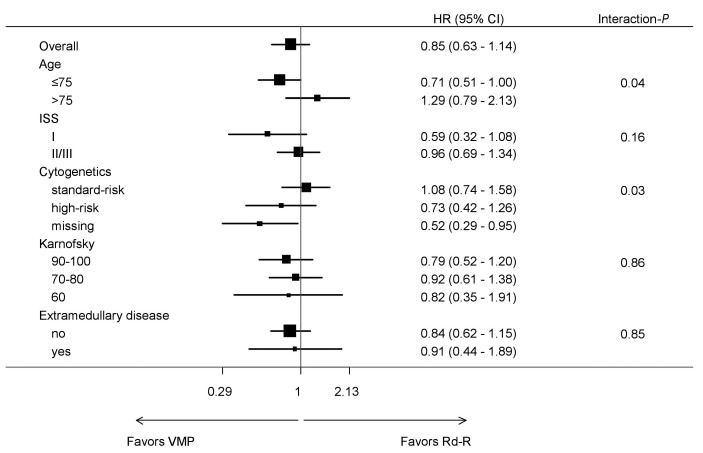
Bortezomib-melphalan-prednisone (VMP) and continuous lenalidomide-dexamethasone (Rd) represent the standard treatment of transplant-ineligible patients with newly diagnosed multiple myeloma (MM). To date, no randomized trial has compared VMP to Rd, and there is no evidence of the optimal treatment for newly diagnosed MM, particularly in patients with high-risk cytogenetics [del(17p), t(4;14) or t(14;16)]. We pooled together data from patients with newly diagnosed MM treated with VMP or Rd induction followed by lenalidomide maintenance 10 mg (Rd-R) enrolled in the GIMEMA-MM-03-05 and EMN01 trials, to evaluate the efficacy of these treatments in different subgroups of patients, focusing on those with standard- and high-risk cytogenetics. Overall, 474 patients were analyzed (VMP: 257 patients; Rd-R: 217 patients). No differences in progression-free survival (hazard ratio=0.96) and overall survival (hazard ratio=1.08) were observed between standard-risk patients treated with VMP or Rd-R, whereas among the high-risk patients, the probabilities of progression (hazard ratio=0.54) and death (hazard ratio=0.73) were lower in the patients treated with VMP than in those treated with Rd-R. In particular, standard-risk patients >75 years benefited less from VMP than from Rd-R (hazard ratio for progression-free survival=0.96; hazard ratio for overall survival=1.81). In this non-randomized analysis, VMP and Rd-R were equally effective in younger (≤75 years), standard-risk patients, while older ones (>75 years) benefited more from Rd-R. In high-risk patients, VMP improved progression-free survival and overall survival irrespective of age. The source trials are registered at ClinicalTrials.gov (NCT01063179 and NCT01093196).
硼替佐米-美法仑-泼尼松(VMP)和连续来那度胺-地塞米松(Rd)是新诊断多发性骨髓瘤(MM)不适合移植患者的标准治疗方法。迄今为止,尚无比较 VMP 与 Rd 的随机试验,也没有新诊断 MM 最佳治疗方法的证据,特别是在具有高危细胞遗传学[del(17p)、t(4;14)或 t(14;16)]的患者中。我们将在 GIMEMA-MM-03-05 和 EMN01 试验中接受 VMP 或 Rd 诱导治疗后接受来那度胺维持治疗 10 mg(Rd-R)的新诊断 MM 患者的数据汇总在一起,以评估这些治疗方法在不同患者亚组中的疗效,重点是标准风险和高风险细胞遗传学患者。共有 474 例患者接受了分析(VMP:257 例;Rd-R:217 例)。在标准风险患者中,VMP 与 Rd-R 治疗的无进展生存期(风险比=0.96)和总生存期(风险比=1.08)无差异,而在高危患者中,VMP 治疗患者的进展(风险比=0.54)和死亡(风险比=0.73)的可能性低于 Rd-R 治疗患者。特别是,75 岁以上的标准风险患者从 VMP 中获益不如 Rd-R(无进展生存期的风险比=0.96;总生存期的风险比=1.81)。在这项非随机分析中,VMP 和 Rd-R 在年轻(≤75 岁)、标准风险患者中同样有效,而年龄较大(>75 岁)的患者则从 Rd-R 中获益更多。在高危患者中,VMP 改善了无进展生存期和总生存期,与年龄无关。原始试验在 ClinicalTrials.gov 注册(NCT01063179 和 NCT01093196)。