Fodor Gergely H, Bayat Sam, Albu Gergely, Lin Na, Baudat Aurélie, Danis Judit, Peták Ferenc, Habre Walid
Unit for Anesthesiological Investigations, Geneva University Hospitals - University of Geneva, Geneva, Switzerland.
Inserm UA7 STROBE Laboratory, Department of Clinical Physiology, Sleep and Exercise, Grenoble University Hospital, Grenoble, France.
Front Physiol. 2019 Jun 26;10:803. doi: 10.3389/fphys.2019.00803. eCollection 2019.
Introducing mathematically derived variability (MVV) into the otherwise monotonous conventional mechanical ventilation has been suggested to improve lung recruitment and gas exchange. Although the application of a ventilation pattern based on variations in physiological breathing (PVV) is beneficial for healthy lungs, its value in the presence of acute respiratory distress syndrome (ARDS) has not been characterized. We therefore aimed at comparing conventional pressure-controlled ventilation with (PCS) or without regular sighs (PCV) to MVV and PVV at two levels of positive end-expiratory pressure (PEEP) in a model of severe ARDS.
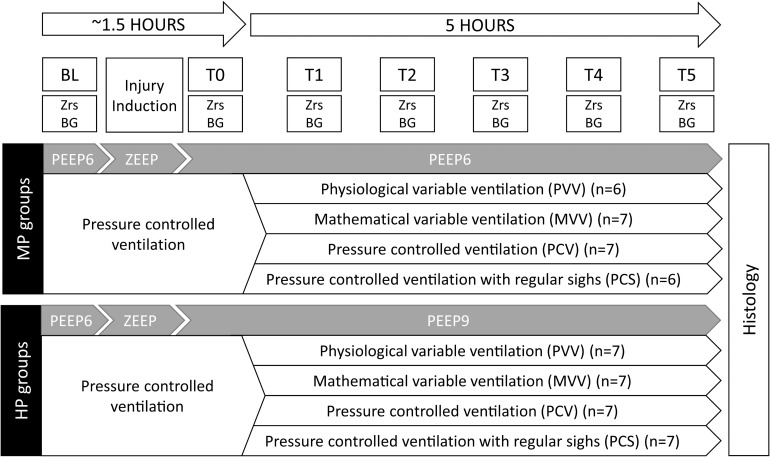
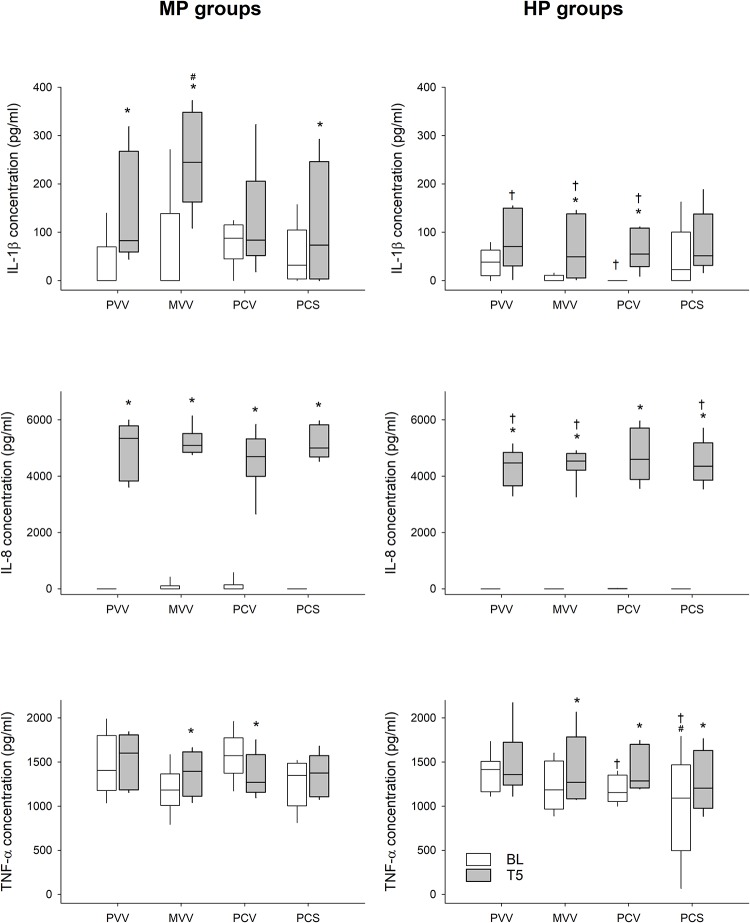
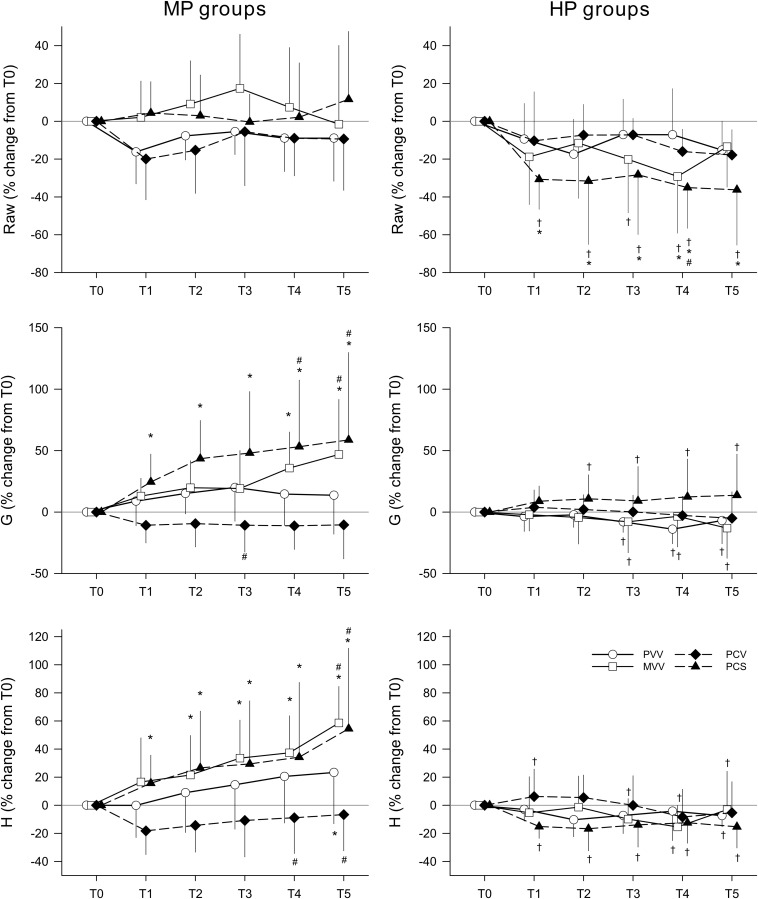
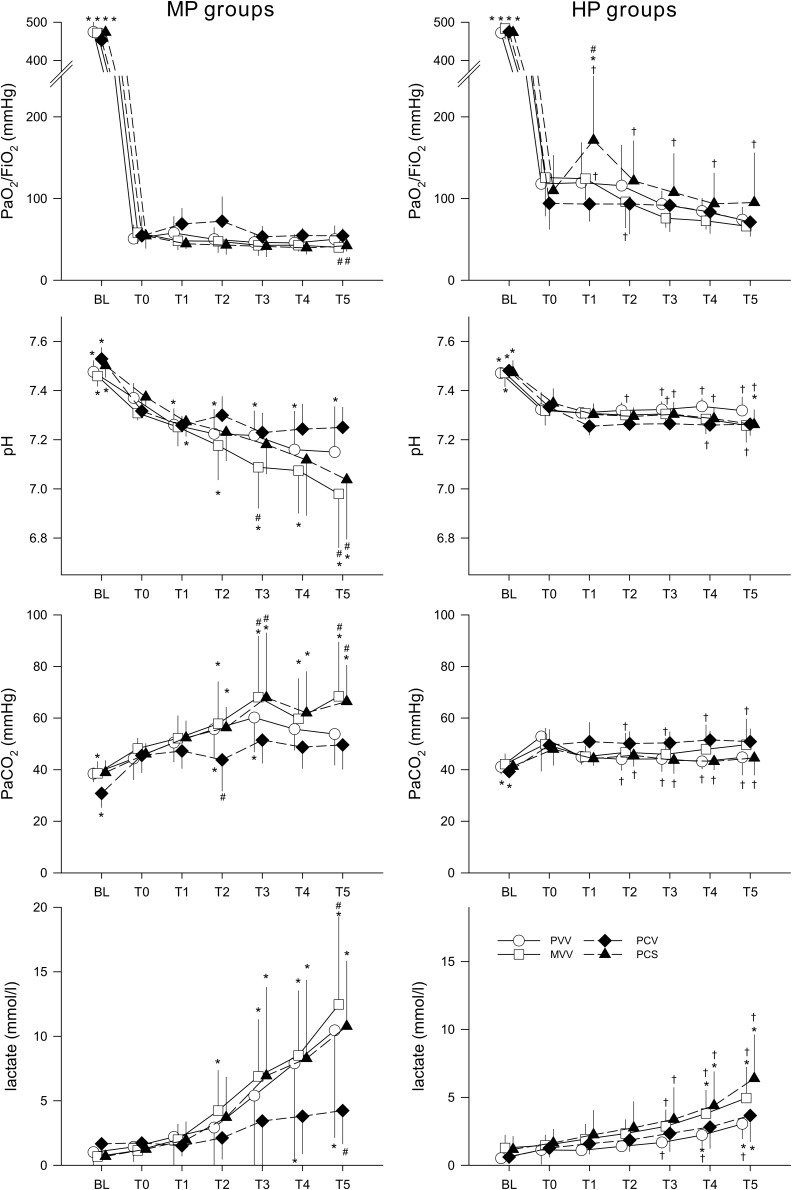
Anesthetised rabbits ( = 54) were mechanically ventilated and severe ARDS (PaO/FiO ≤ 150 mmHg) was induced by combining whole lung lavage, i.v. endotoxin and injurious ventilation. Rabbits were then randomly assigned to be ventilated with PVV, MVV, PCV, or PCS for 5 h while maintaining either 6 or 9 cmHO PEEP. Ventilation parameters, blood gas indices and respiratory mechanics (tissue damping, G, and elastance, H) were recorded hourly. Serum cytokine levels were assessed with ELISA and lung histology was analyzed.
Although no progression of lung injury was observed after 5 h of ventilation at PEEP 6 cmHO with PVV and PCV, values for G (58.8 ± 71.1[half-width of 95% CI]% and 40.8 ± 39.0%, respectively), H (54.5 ± 57.2%, 50.7 ± 28.3%), partial pressure of carbon-dioxide (PaCO, 43.9 ± 23.8%, 46.2 ± 35.4%) and pH (-4.6 ± 3.3%, -4.6 ± 2.2%) worsened with PCS and MVV. Regardless of ventilation pattern, application of a higher PEEP improved lung function and precluded progression of lung injury and inflammation. Histology lung injury scores were elevated in all groups with no difference between groups at either PEEP level.
At moderate PEEP, variable ventilation based on a pre-recorded physiological breathing pattern protected against progression of lung injury equally to the conventional pressure-controlled mode, whereas mathematical variability or application of regular sighs caused worsening in lung mechanics. This outcome may be related to the excessive increases in peak inspiratory pressure with the latter ventilation modes. However, a greater benefit on respiratory mechanics and gas exchange could be obtained by elevating PEEP, compared to the ventilation mode in severe ARDS.
有人提出在原本单调的传统机械通气中引入数学推导的变异性(MVV),以改善肺复张和气体交换。尽管基于生理呼吸变化(PVV)的通气模式对健康肺有益,但其在急性呼吸窘迫综合征(ARDS)中的价值尚未明确。因此,我们旨在比较在严重ARDS模型中,在两个呼气末正压(PEEP)水平下,常规压力控制通气(带规律叹息,PCS;不带规律叹息,PCV)与MVV和PVV的效果。
对54只麻醉兔进行机械通气,通过全肺灌洗、静脉注射内毒素和有害通气诱导严重ARDS(动脉血氧分压/吸入氧分数值≤150 mmHg)。然后将兔随机分为接受PVV、MVV、PCV或PCS通气5小时,同时维持6 cmH₂O或9 cmH₂O的PEEP。每小时记录通气参数、血气指标和呼吸力学参数(组织阻尼,G;弹性,H)。用酶联免疫吸附测定法评估血清细胞因子水平,并分析肺组织学。
在6 cmH₂O的PEEP下,采用PVV和PCV通气5小时后未观察到肺损伤进展,而PCS和MVV组的G值(分别为58.8±71.1[95%置信区间半宽]%和40.8±39.0%)、H值(54.5±57.2%,50.7±2
8.3%)、二氧化碳分压(PaCO₂,43.9±23.8%,46.2±35.4%)和pH值(-4.6±3.3%,-4.6±2.2%)恶化。无论通气模式如何,采用较高的PEEP可改善肺功能,防止肺损伤和炎症进展。所有组的肺组织学损伤评分均升高,在任一PEEP水平下各组间无差异。
在中度PEEP水平,基于预先记录的生理呼吸模式的可变通气对防止肺损伤进展的保护作用与传统压力控制模式相同,而数学变异性或规律叹息的应用会导致肺力学恶化。这一结果可能与后两种通气模式下吸气峰压过度升高有关。然而,与严重ARDS的通气模式相比,提高PEEP对呼吸力学和气体交换可能有更大益处。