Henssen Dylan Jozef Hendrik Augustinus, Weber Rosanna Christina, de Boef Jesse, Mollink Jeroen, Kozicz Tamas, Kurt Erkan, van Cappellen van Walsum Anne-Marie
Department of Anatomy, Donders Institute for Brain, Cognition & Behavior, Radboud University Medical Center, Nijmegen, Netherlands.
Unit of Functional Neurosurgery, Department of Neurosurgery, Radboud University Medical Center, Nijmegen, Netherlands.
Front Neuroanat. 2019 Jul 2;13:66. doi: 10.3389/fnana.2019.00066. eCollection 2019.
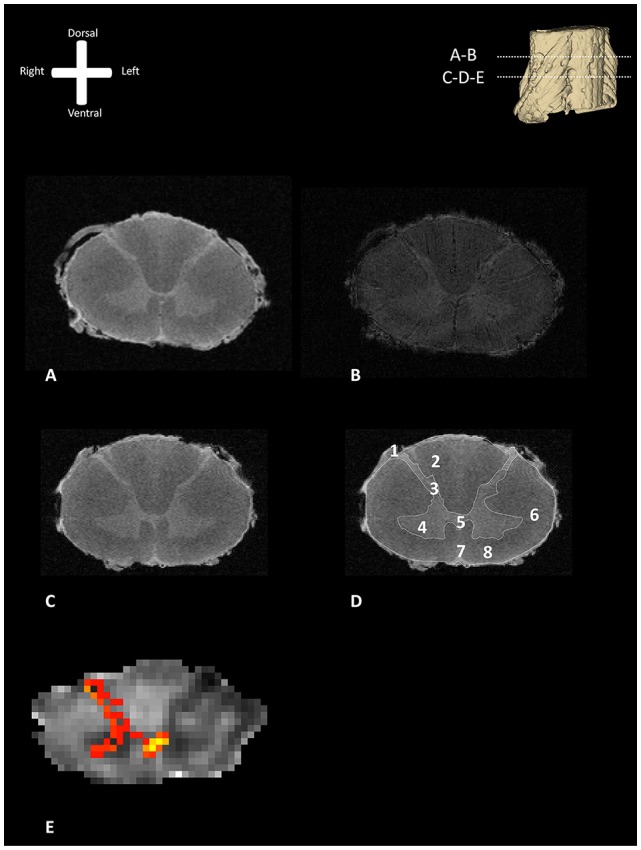
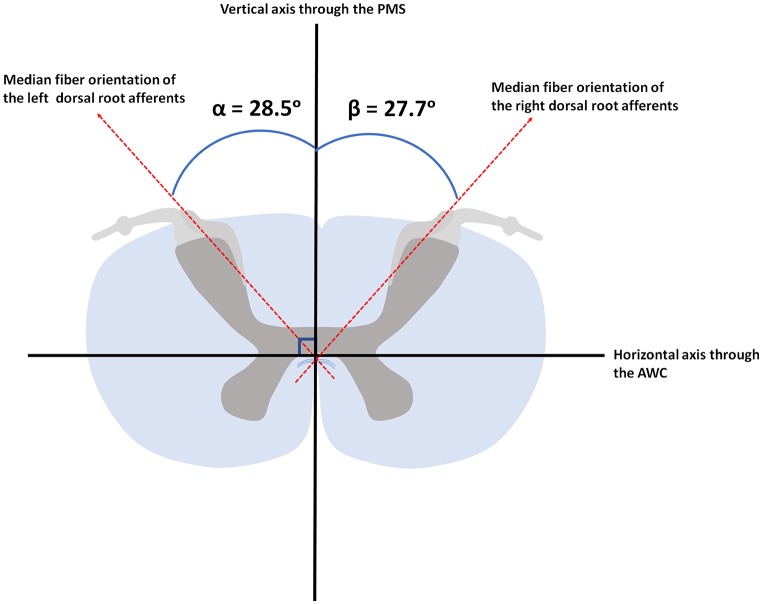
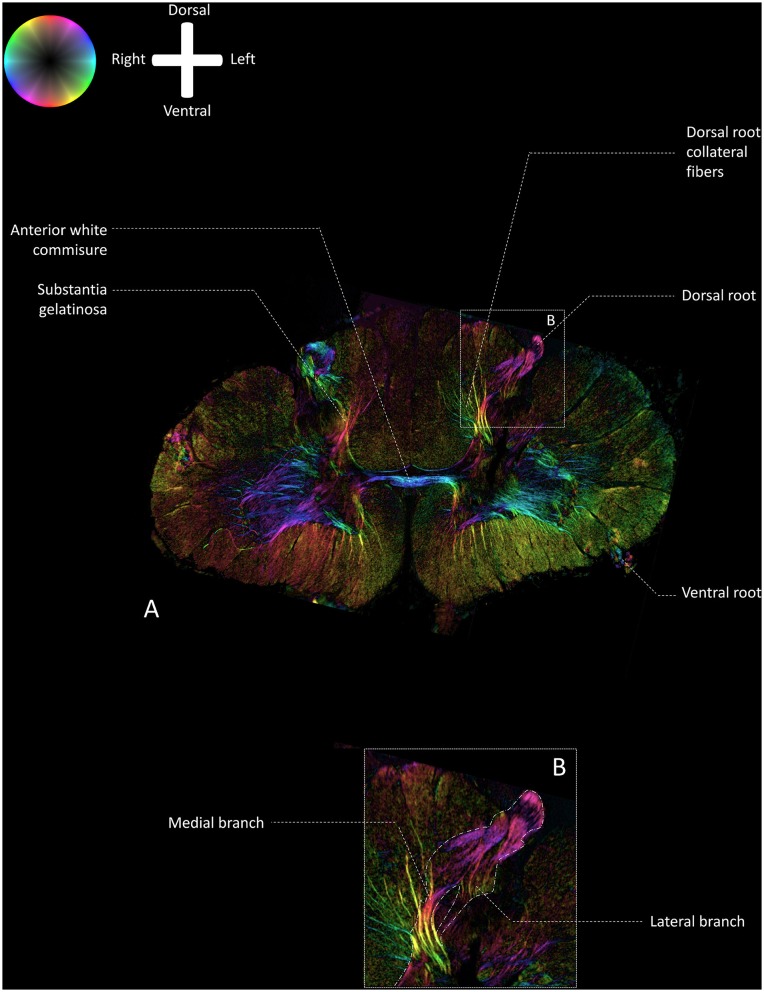
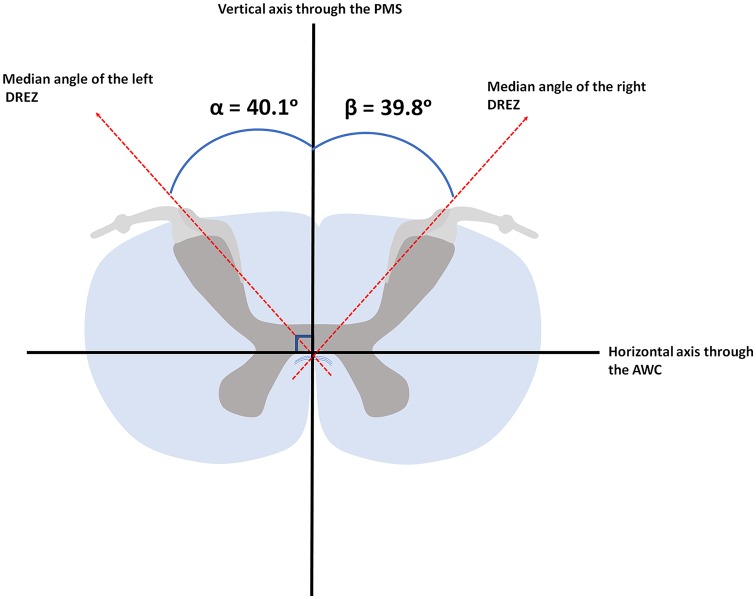
: Destruction of the afferents by dorsal root entry zone (DREZ) surgery may be an effective treatment of intractable neuropathic pain, though it remains a high-risk surgical intervention. Potential complications due to the lesioning of structures within the cervical spinal cord other than the DREZ can be minimized by accurate knowledge of the optimal insertion angle [i.e., the angle between the DREZ and the posterior median sulcus (PMS)]. The employed insertion angle was based on measurements between the DREZ and the PMS on post-mortem transverse slices. However, new, more sophisticated imaging techniques are currently available and are thought to yield higher spatial resolution and more accurate images. : This article measures the angle between the DREZ and the PMS on 11.7T post-mortem magnetic resonance images and compares these findings with polarized light imaging (PLI) microscopy images of the same specimens in order to quantify fiber orientation within the DREZ. : To visualize the anatomy of the cervical DREZ, magnetic resonance imaging (MRI), diffusion-weighted MRI (dMRI), probabilistic tractography, and PLI were performed on three post-mortem human cervical spinal cords at level C5-C6. The MR data was used to measure the angle between the DREZ and the PMS. MR images were complemented by probabilistic tractography results. Then, the orientation of fibers within the DREZ was quantified by use of PLI microscopy. : Median angle between the DREZ and the PMS, as measured on MR-images, was found to be 40.1° (ranging from 34.2° to 49.1°) and 39.8° (ranging from 31.1° to 47.8°) in the left and right hemicord, respectively. Median fiber orientation within the DREZ, as quantified by PLI, was 28.5° (ranging from 12.0° to 44.3°) and 27.7° (ranging from 8.5° to 38.1°) in the left and right hemicord, respectively. : Our study, which provides an improved understanding of the anatomy of the DREZ, the angle between the DREZ and the PMS and the median fiber orientation within the DREZ, could contribute to safer DREZ-lesioning surgery to treat chronic neuropathic pain in the future.
通过背根入髓区(DREZ)手术破坏传入神经可能是治疗顽固性神经性疼痛的一种有效方法,尽管它仍然是一种高风险的外科干预措施。通过准确了解最佳插入角度[即DREZ与后正中沟(PMS)之间的角度],可将因损伤颈髓内DREZ以外的结构而导致的潜在并发症降至最低。所采用的插入角度是基于对死后横切片上DREZ与PMS之间的测量。然而,目前已有更新的、更先进的成像技术,据认为这些技术能产生更高的空间分辨率和更精确的图像。本文在11.7T死后磁共振图像上测量DREZ与PMS之间的角度,并将这些结果与相同标本的偏振光成像(PLI)显微镜图像进行比较,以便量化DREZ内的纤维方向。为了可视化颈段DREZ的解剖结构,对三个死后人体颈髓C5 - C6节段进行了磁共振成像(MRI)、扩散加权MRI(dMRI)、概率性纤维束成像和PLI检查。利用MR数据测量DREZ与PMS之间的角度。MR图像辅以概率性纤维束成像结果。然后,通过PLI显微镜量化DREZ内纤维的方向。在MR图像上测量发现,左侧和右侧半脊髓中DREZ与PMS之间的中位角度分别为40.1°(范围为34.2°至49.1°)和39.8°(范围为31.1°至47.8°)。通过PLI量化,左侧和右侧半脊髓中DREZ内纤维的中位方向分别为28.5°(范围为12.0°至44.3°)和27.7°(范围为8.5°至38.1°)。我们的研究有助于更好地理解DREZ的解剖结构、DREZ与PMS之间的角度以及DREZ内纤维的中位方向,可能有助于未来更安全地进行DREZ毁损手术以治疗慢性神经性疼痛。