Cao Christopher, Louie Brian E, Melfi Franca, Veronesi Giulia, Razzak Rene, Romano Gaetano, Novellis Pierluigi, Ranganath Neel K, Park Bernard J
Department of Surgery, Thoracic Service, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Department of Cardiothoracic Surgery, Royal Prince Alfred Hospital, Sydney, NSW, Australia.
Eur J Cardiothorac Surg. 2020 Feb 1;57(2):338-342. doi: 10.1093/ejcts/ezz205.
Percentage-predicted forced expiratory volume in 1 s (FEV1) and diffusing capacity for carbon monoxide (DLCO), and their predicted postoperative (ppo) values are established prognostic factors for postoperative pulmonary complications after thoracotomy. However, their predictive value for minimally invasive pulmonary resections remains controversial. This study assessed the incidence of pulmonary complications after robotic lobectomy for primary lung cancer and analysed the predictive significance of FEV1 and DLCO.
This was a retrospective analysis of patients who underwent robotic lobectomy from 4 institutions. Descriptive and comparative analyses were performed for patients who experienced pulmonary complications versus patients who did not, in relation to FEV1 and DLCO values. To identify thresholds for increased complications, patients were categorized into groups of 10% incremental increases in FEV1 and DLCO, and their ppo values.
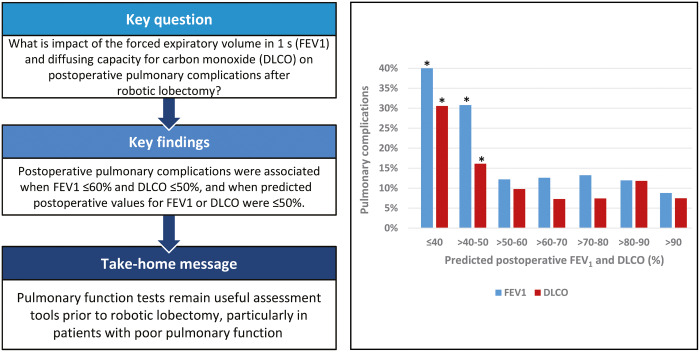
From November 2002 to April 2018, 1088 patients underwent robotic lobectomy. Overall, 169 postoperative pulmonary complications occurred in 141 patients. Male gender and Eastern Cooperative Oncology Group grade ≥1 were associated with increased pulmonary complications on univariable analysis. Patients who experienced pulmonary complications had increased mortality (2.1% vs 0.2%, P = 0.017) and longer hospitalizations (9 vs 4 days, P < 0.001). Pulmonary complications were associated when FEV1 ≤60% and DLCO ≤50%, and when ppo FEV1 or DLCO was ≤50%; ppo FEV1 ≤50% (P < 0.001) and ppo DLCO ≤50% (P = 0.031) remained statistically significant on multivariable analysis.
Both FEV1 and DLCO were shown to be significant predictors of pulmonary complications. Furthermore, thresholds of percentage-predicted and ppo FEV1 and DLCO values were identified, below which pulmonary complications occurred significantly more frequently, suggesting their predictive values are particularly useful in patients with poorer pulmonary function.
一秒用力呼气容积(FEV1)和一氧化碳弥散量(DLCO)的预测百分比及其术后预测值是开胸术后肺部并发症的既定预后因素。然而,它们对微创肺切除术的预测价值仍存在争议。本研究评估了原发性肺癌机器人肺叶切除术后肺部并发症的发生率,并分析了FEV1和DLCO的预测意义。
这是一项对来自4家机构接受机器人肺叶切除术患者的回顾性分析。对发生肺部并发症的患者与未发生肺部并发症的患者的FEV1和DLCO值进行描述性和比较性分析。为了确定并发症增加的阈值,将患者按照FEV1和DLCO及其术后预测值以10%的增量递增进行分组。
2002年11月至2018年4月,1088例患者接受了机器人肺叶切除术。总体而言,141例患者发生了169例术后肺部并发症。单因素分析显示,男性和东部肿瘤协作组(ECOG)分级≥1与肺部并发症增加相关。发生肺部并发症的患者死亡率更高(2.1%对0.2%,P = 0.017),住院时间更长(9天对4天,P < 0.001)。当FEV1≤60%且DLCO≤50%时,以及当术后预测FEV1或DLCO≤50%时,与肺部并发症相关;多因素分析显示,术后预测FEV1≤50%(P < 0.001)和术后预测DLCO≤50%(P = 0.031)仍具有统计学意义。
FEV1和DLCO均被证明是肺部并发症的重要预测指标。此外,确定了预测百分比以及术后预测FEV1和DLCO值的阈值,低于这些阈值时肺部并发症发生频率显著更高,表明它们的预测价值在肺功能较差的患者中特别有用。