Salibian Ara A, Frey Jordan D, Bekisz Jonathan M, Karp Nolan S, Choi Mihye
Hansjörg Wyss Department of Plastic Surgery, New York University Langone Health; New York, N.Y.
Plast Reconstr Surg Glob Open. 2019 May 23;7(5):e2280. doi: 10.1097/GOX.0000000000002280. eCollection 2019 May.
Mastectomy flap and nipple-areola complex (NAC) ischemia can be devastating complications after nipple-sparing mastectomy (NSM). Predictors of reconstructive failure with major skin envelope ischemia and implications for decision-making remain to be fully elucidated.
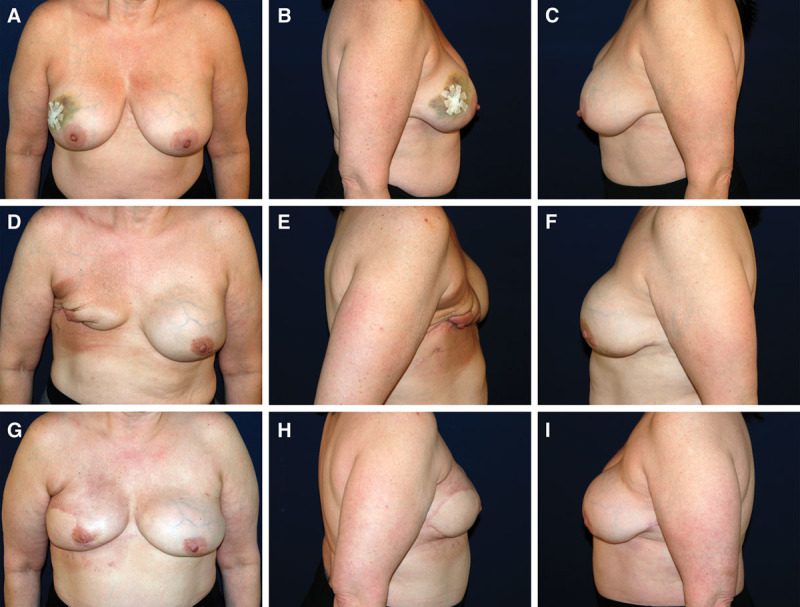
All cases of implant-based reconstruction after NSM from 2006 to June 2018 with mastectomy flap necrosis or NAC necrosis requiring debridement were reviewed. Data on patient demographics, operative characteristics, additional complications, and the nature and management of ischemic complications were collected and analyzed.
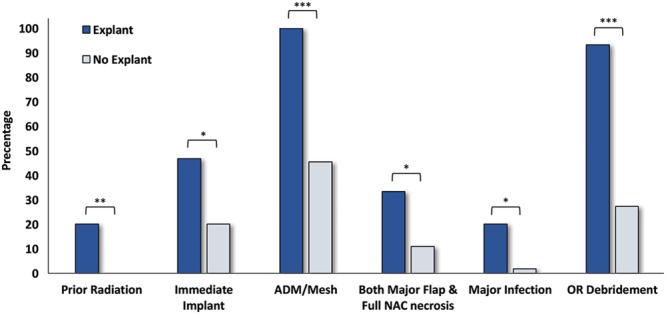
Out of 1045 NSMs, 70 cases (6.7%) had major ischemic complications. Fifty-two cases (74.3% of major ischemic complications) had isolated major mastectomy flap necrosis, 7 (10%) had full NAC necrosis and 11 (15.7%) had both. Five cases (7.1%) underwent implant exchange at the time of debridement and 15 cases (21.4%) required explantation. Explanted cases had significantly lower body mass index (22.3 versus 24.7, = 0.013) and larger debridement size (49.5 cm versus 17.6 cm, = 0.0168). Additionally, explanted cases had a higher rate of acellular dermal matrix/mesh (100% versus 45.5%, < 0.0001), prior radiation (20.0% versus 0%, = 0.0083), immediate implants (46.7% versus 20.0%, = 0.0491), major infection (30.0% versus 1.8%, = 0.028), and both major mastectomy flap/NAC necrosis (33.3% versus 10.9%, = 0.0494).
NSM cases with major ischemia requiring explantation had a lower body mass index and significantly higher rate of preoperative radiation, immediate implant placement, use of acellular dermal matrix/mesh, and concomitant major infection. These variables should be taken into account when discussing risks with patients preoperatively and assessing the quality of mastectomy flaps and subsequent reconstructive choices intraoperatively.
保留乳头的乳房切除术(NSM)后,乳房切除皮瓣和乳头乳晕复合体(NAC)缺血可能是毁灭性的并发症。主要皮肤包膜缺血导致重建失败的预测因素及其对决策的影响仍有待充分阐明。
回顾了2006年至2018年6月所有NSM后采用植入物重建且因乳房切除皮瓣坏死或NAC坏死需要清创的病例。收集并分析了患者人口统计学数据、手术特征、其他并发症以及缺血性并发症的性质和处理情况。
在1045例NSM中,70例(6.7%)发生了严重缺血性并发症。52例(严重缺血性并发症的74.3%)仅有乳房切除皮瓣严重坏死,7例(10%)NAC完全坏死,11例(15.7%)两者均有。5例(7.1%)在清创时进行了植入物更换,15例(21.4%)需要取出植入物。取出植入物的病例体重指数显著较低(22.3对24.7,P = 0.013),清创面积较大(49.5平方厘米对17.6平方厘米,P = 0.0168)。此外,取出植入物的病例使用脱细胞真皮基质/网片的比例更高(100%对45.5%,P < 0.0001),既往接受过放疗的比例更高(20.0%对0%,P = 0.0083),即刻植入的比例更高(46.7%对20.0%,P = 0.0,491),发生严重感染的比例更高(30.0%对1.8%,P = 0.028),乳房切除皮瓣/NAC均严重坏死的比例更高(33.3%对10.9%,P = 0.0494)。
需要取出植入物的严重缺血性NSM病例体重指数较低,术前放疗、即刻植入、使用脱细胞真皮基质/网片以及并发严重感染的比例显著更高。在术前与患者讨论风险以及术中评估乳房切除皮瓣质量和后续重建选择时,应考虑这些变量。