Borensztajn Dorine, Yeung Shunmay, Hagedoorn Nienke N, Balode Anda, von Both Ulrich, Carrol Enitan D, Dewez Juan Emmanuel, Eleftheriou Irini, Emonts Marieke, van der Flier Michiel, de Groot Ronald, Herberg Jethro Adam, Kohlmaier Benno, Lim Emma, Maconochie Ian, Martinón-Torres Federico, Nijman Ruud, Pokorn Marko, Strle Franc, Tsolia Maria, Wendelin Gerald, Zavadska Dace, Zenz Werner, Levin Michael, Moll Henriette A
Department of General Paediatrics, Erasmus MC-Sophia Children's Hospital, Rotterdam, The Netherlands.
Faculty of Infectious and Tropical Disease, London School of Hygiene and Tropical Medicine, London, UK.
BMJ Paediatr Open. 2019 Jun 27;3(1):e000456. doi: 10.1136/bmjpo-2019-000456. eCollection 2019.
To provide an overview of care in emergency departments (EDs) across Europe in order to interpret observational data and implement interventions regarding the management of febrile children.
An electronic questionnaire was sent to the principal investigators of an ongoing study (PERFORM (Personalised Risk assessment in Febrile illness to Optimise Real-life Management), www.perform2020.eu) in 11 European hospitals in eight countries: Austria, Germany, Greece, Latvia, the Netherlands, Slovenia, Spain and the UK.
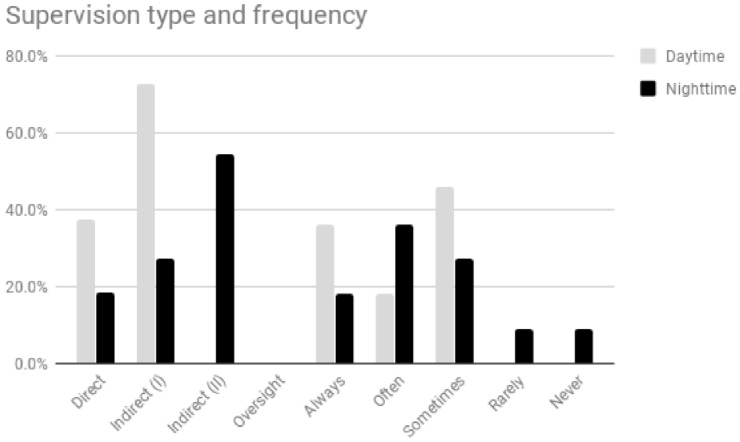
The questionnaire covered indicators in three domains: local ED quality (supervision, guideline availability, paper vs electronic health records), organisation of healthcare (primary care, immunisation), and local factors influencing or reflecting resource use (availability of point-of-care tests, admission rates).
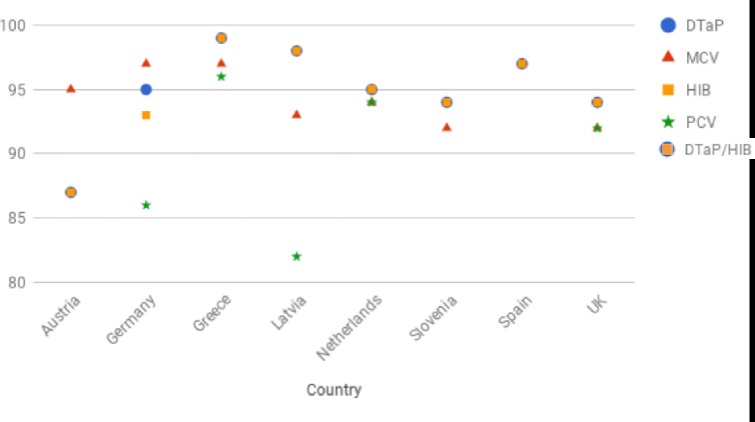
Reported admission rates ranged from 4% to 51%. In six settings (Athens, Graz, Ljubljana, Riga, Rotterdam, Santiago de Compostela), the supervising ED physicians were general paediatricians, in two (Liverpool, London) these were paediatric emergency physicians, in two (Nijmegen, Newcastle) supervision could take place by either a general paediatrician or a general emergency physician, and in one (München) this could be either a general paediatrician or a paediatric emergency physician. The supervising physician was present on site in all settings during office hours and in five out of eleven settings during out-of-office hours. Guidelines for fever and sepsis were available in all settings; however, the type of guideline that was used differed. Primary care was available in all settings during office hours and in eight during out-of-office hours. There were differences in routine immunisations as well as in additional immunisations that were offered; immunisation rates varied between and within countries.
Differences in local, regional and national aspects of care exist in the management of febrile children across Europe. This variability has to be considered when trying to interpret differences in the use of diagnostic tools, antibiotics and admission rates. Any future implementation of interventions or diagnostic tests will need to be aware of this European diversity.
概述欧洲各地急诊科的护理情况,以便解读观察数据并实施有关发热儿童管理的干预措施。
向八个国家11家欧洲医院(奥地利、德国、希腊、拉脱维亚、荷兰、斯洛文尼亚、西班牙和英国)正在进行的一项研究(PERFORM(发热疾病的个性化风险评估以优化实际管理),www.perform2020.eu)的主要研究者发送了一份电子问卷。
问卷涵盖三个领域的指标:当地急诊科质量(监督、指南可用性、纸质与电子健康记录)、医疗保健组织(初级保健、免疫接种)以及影响或反映资源使用的当地因素(即时检验可用性、住院率)。
报告的住院率在4%至51%之间。在六个地点(雅典、格拉茨、卢布尔雅那、里加、鹿特丹、圣地亚哥 - 德孔波斯特拉),急诊科的监督医师为普通儿科医生;在两个地点(利物浦和伦敦),这些是儿科急诊医师;在两个地点(奈梅亨、纽卡斯尔),监督可由普通儿科医生或普通急诊医师进行;在一个地点(慕尼黑),这可以是普通儿科医生或儿科急诊医师。监督医师在办公时间内在所有地点都在场,在非办公时间内在11个地点中的5个地点在场。所有地点都有发热和脓毒症指南;然而,所使用的指南类型有所不同。办公时间内所有地点都有初级保健服务,非办公时间内有8个地点有。常规免疫接种以及提供的额外免疫接种存在差异;免疫接种率在不同国家之间以及国家内部各不相同。
欧洲各地发热儿童管理在地方、区域和国家层面的护理存在差异。在试图解读诊断工具、抗生素使用和住院率差异时,必须考虑这种变异性。未来任何干预措施或诊断测试的实施都需要意识到这种欧洲范围内的多样性。