Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts (C.V.D., S.S., D.K., M.F., A.T., E.P.).
Ann Intern Med. 2019 Aug 20;171(4):248-256. doi: 10.7326/M18-3136. Epub 2019 Jul 30.
Prior studies evaluating risk for severe urinary tract infections (UTIs) with sodium-glucose cotransporter-2 (SGLT-2) inhibitors have reported conflicting findings.
To assess whether patients initiating use of SGLT-2 inhibitors were at increased risk for severe UTI events compared with those initiating use of dipeptidyl peptidase-4 (DPP-4) inhibitors or glucagon-like peptide-1 receptor (GLP-1) agonists.
Population-based cohort study.
2 large, U.S.-based databases of commercial claims (March 2013 to September 2015).
Within each database, 2 cohorts were created and matched 1:1 on propensity score. Patients were aged 18 years or older, had type 2 diabetes mellitus, and were initiating use of SGLT-2 inhibitors versus DPP-4 inhibitors (cohort 1) or GLP-1 agonists (cohort 2).
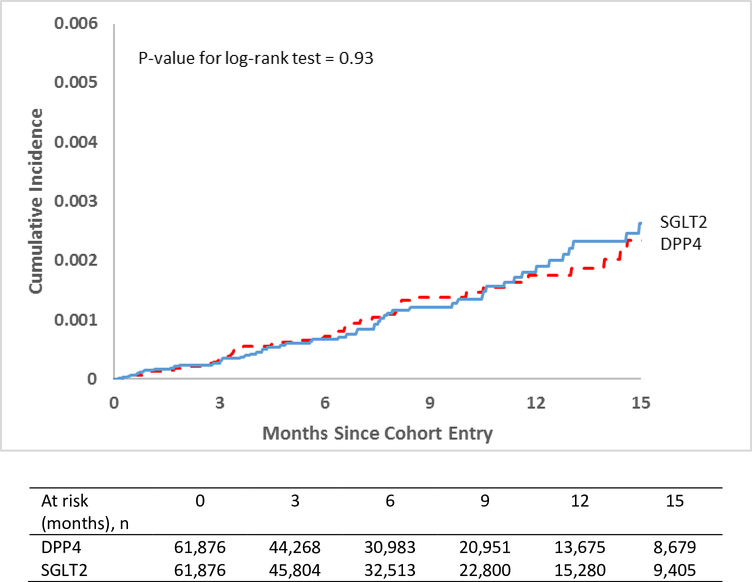
The primary outcome was a severe UTI event, defined as a hospitalization for primary UTI, sepsis with UTI, or pyelonephritis; the secondary outcome was outpatient UTI treated with antibiotics. Hazard ratios (HRs) were estimated in each propensity score-matched cohort, with adjustment for more than 90 baseline characteristics.
After 1:1 matching on propensity score, 123 752 patients were identified in cohort 1 and 111 978 in cohort 2 in the 2 databases. In cohort 1, persons newly receiving SGLT-2 inhibitors had 61 severe UTI events (incidence rate [IR] per 1000 person-years, 1.76), compared with 57 events in the DPP-4 inhibitor group (IR, 1.77) (HR, 0.98 [95% CI, 0.68 to 1.41]). In cohort 2, those receiving SGLT-2 inhibitors had 73 events (IR, 2.15), compared with 87 events in the GLP-1 agonist group (IR, 2.96) (HR, 0.72 [CI, 0.53 to 0.99]). Findings were robust across sensitivity analyses; within several subgroups of age, sex, and frailty; and for canagliflozin and dapagliflozin individually. In addition, SGLT-2 inhibitors were not associated with increased risk for outpatient UTIs (cohort 1: HR, 0.96 [CI, 0.89 to 1.04]; cohort 2: HR, 0.91 [CI, 0.84 to 0.99]).
Generalizability of the study findings may be limited to patients with commercial insurance.
In a large cohort of patients seen in routine clinical practice, risk for severe and nonsevere UTI events among those initiating SGLT-2 inhibitor therapy was similar to that among patients initiating treatment with other second-line antidiabetic medications.
Brigham and Women's Hospital, Division of Pharmacoepidemiology and Pharmacoeconomics.
先前评估钠-葡萄糖协同转运蛋白 2(SGLT-2)抑制剂治疗严重尿路感染(UTI)风险的研究结果存在矛盾。
评估与起始使用二肽基肽酶-4(DPP-4)抑制剂或胰高血糖素样肽-1 受体(GLP-1)激动剂相比,起始使用 SGLT-2 抑制剂的患者发生严重 UTI 事件的风险是否增加。
基于人群的队列研究。
2 个美国大型商业索赔数据库(2013 年 3 月至 2015 年 9 月)。
在每个数据库中,创建了 2 个队列,并按倾向评分进行 1:1 匹配。患者年龄≥18 岁,患有 2 型糖尿病,起始使用 SGLT-2 抑制剂与 DPP-4 抑制剂(队列 1)或 GLP-1 激动剂(队列 2)。
主要结局是严重 UTI 事件,定义为因原发性 UTI、UTI 合并败血症或肾盂肾炎住院治疗;次要结局是门诊使用抗生素治疗的 UTI。在每个倾向评分匹配的队列中,使用调整了 90 多项基线特征的风险比(HR)进行估计。
在 2 个数据库中,1:1 倾向评分匹配后,队列 1 中确定了 123752 例患者,队列 2 中确定了 111978 例患者。在队列 1 中,新接受 SGLT-2 抑制剂治疗的患者发生 61 例严重 UTI 事件(发病率[IR]为每 1000 人年 1.76),而 DPP-4 抑制剂组为 57 例事件(IR,1.77)(HR,0.98[95%CI,0.68 至 1.41])。在队列 2 中,接受 SGLT-2 抑制剂治疗的患者发生 73 例事件(IR,2.15),而 GLP-1 激动剂组为 87 例事件(IR,2.96)(HR,0.72[CI,0.53 至 0.99])。敏感性分析结果稳健;在年龄、性别和脆弱性等多个亚组中;对于坎格列净和达格列净分别进行分析。此外,SGLT-2 抑制剂与门诊 UTI 风险增加无关(队列 1:HR,0.96[CI,0.89 至 1.04];队列 2:HR,0.91[CI,0.84 至 0.99])。
研究结果的推广性可能仅限于有商业保险的患者。
在常规临床实践中观察到的大型患者队列中,起始 SGLT-2 抑制剂治疗的患者与起始使用其他二线抗糖尿病药物治疗的患者发生严重和非严重 UTI 事件的风险相似。
布莱根妇女医院,药物流行病学和药物经济学部。