The Demographic and Health Surveys (DHS) Program, ICF, 530 Gaither Road, Suite 500, Rockville, MD, 20850, USA.
U.S. President's Malaria Initiative, USAID, Washington, DC, USA.
Malar J. 2019 Jul 29;18(1):258. doi: 10.1186/s12936-019-2892-x.
Ensuring universal access to malaria diagnosis and treatment is a key component of Pillar 1 of the World Health Organization Global Technical Strategy for Malaria 2016-2030. To achieve this goal it is essential to know the types of facilities where the population seeks care as well as the malaria service readiness of these facilities in endemic countries.
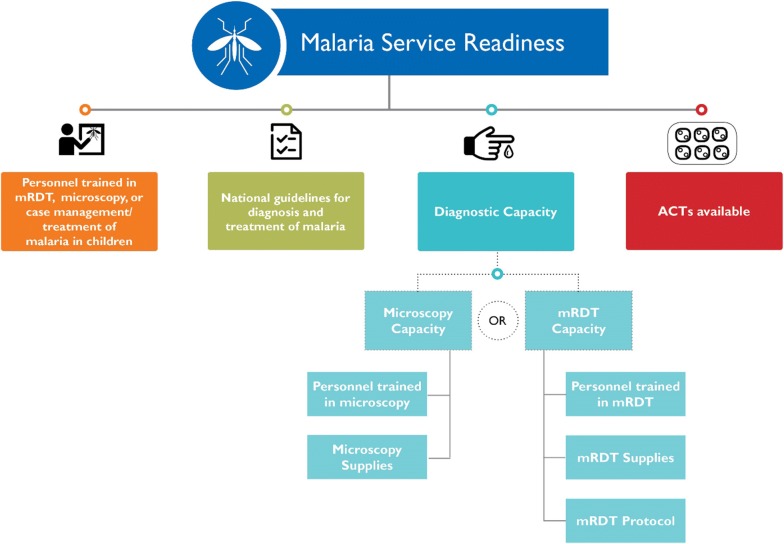
To investigate the utilization and provision of malaria services, data on the sources of advice or treatment in children under 5 years with fever from the household-based Demographic and Health Surveys (DHS) and on the components of malaria service readiness from the facility-based Service Provision Assessment (SPA) surveys were examined in Malawi, Senegal and Tanzania. Facilities categorized as malaria-service ready were those with: (1) personnel trained in either malaria rapid diagnostic testing (RDT), microscopy or case management/treatment of malaria in children; (2) national guidelines for the diagnosis and treatment of malaria; (3) diagnostic capacity (available RDT tests or microscopy equipment as well as staff trained in its use); and, (4) unexpired artemisinin-based combination therapy (ACT) available on the day of the survey.
In all three countries primary-level facilities (health centre/health post/health clinic) were the type of facility most used for care of febrile children. However, only 69% of these facilities in Senegal, 32% in Malawi and 19% in Tanzania were classified as malaria-service ready. Of the four components of malaria-service readiness in the facilities most frequented by febrile children, diagnostic capacity was the weakest area in all three countries, followed by trained personnel. All three countries performed well in the availability of ACT.
This analysis highlights the need to improve the malaria-service readiness of facilities in all three countries. More effort should be focused on facilities that are commonly used for care of fever, especially in the areas of malaria diagnostic capacity and provider training. It is essential for policymakers to consider the malaria-service readiness of primary healthcare facilities when allocating resources. This is particularly important in limited-resource settings to ensure that the facilities most visited for care are properly equipped to provide diagnosis and treatment for malaria.
确保全民获得疟疾诊断和治疗服务是 2016-2030 年世界卫生组织全球疟疾技术战略支柱 1 的关键组成部分。要实现这一目标,必须了解人们寻求医疗服务的设施类型,以及流行国家这些设施的疟疾服务准备情况。
为了调查疟疾服务的利用和提供情况,我们检查了来自基于家庭的人口与健康调查(DHS)的 5 岁以下发热儿童就诊来源数据,以及来自基于设施的服务提供评估(SPA)调查的疟疾服务准备情况数据。被归类为疟疾服务准备就绪的设施应具备以下条件:(1)经过疟疾快速诊断检测(RDT)、显微镜检查或儿童疟疾病例管理/治疗培训的人员;(2)国家疟疾诊断和治疗指南;(3)诊断能力(可用的 RDT 检测或显微镜设备以及经过培训的人员);以及,(4)在调查当天有未过期的青蒿素为基础的联合疗法(ACT)。
在所有三个国家,基层卫生保健设施(保健中心/保健站/诊所)是用于治疗发热儿童的最常用的设施类型。然而,塞内加尔、马拉维和坦桑尼亚的这类设施中仅有 69%、32%和 19%被归类为疟疾服务准备就绪。在发热儿童最常去的设施的疟疾服务准备情况的四个组成部分中,诊断能力在所有三个国家都是最薄弱的环节,其次是培训人员。所有三个国家在 ACT 的供应方面表现良好。
这项分析突出表明需要提高所有三个国家的设施疟疾服务准备情况。应更加关注常用于治疗发热的设施,特别是在疟疾诊断能力和提供者培训方面。政策制定者在分配资源时必须考虑基层卫生保健设施的疟疾服务准备情况。在资源有限的环境中,这一点尤为重要,以确保为医疗服务而就诊的设施配备适当的设备,以便提供疟疾诊断和治疗。