Wong Kerry Lm, Brady Oliver J, Campbell Oona Maeve Renee, Jarvis Christopher I, Pembe Andrea, Gomez Gabriela B, Benova Lenka
Infectious Disease and Epidemiology, London School of Hygiene and Tropical Medicine Faculty of Epidemiology and Population Health, London, UK.
Centre for Mathematical Modelling for Infectious Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom.
BMJ Glob Health. 2019 Aug 21;4(4):e001552. doi: 10.1136/bmjgh-2019-001552. eCollection 2019.
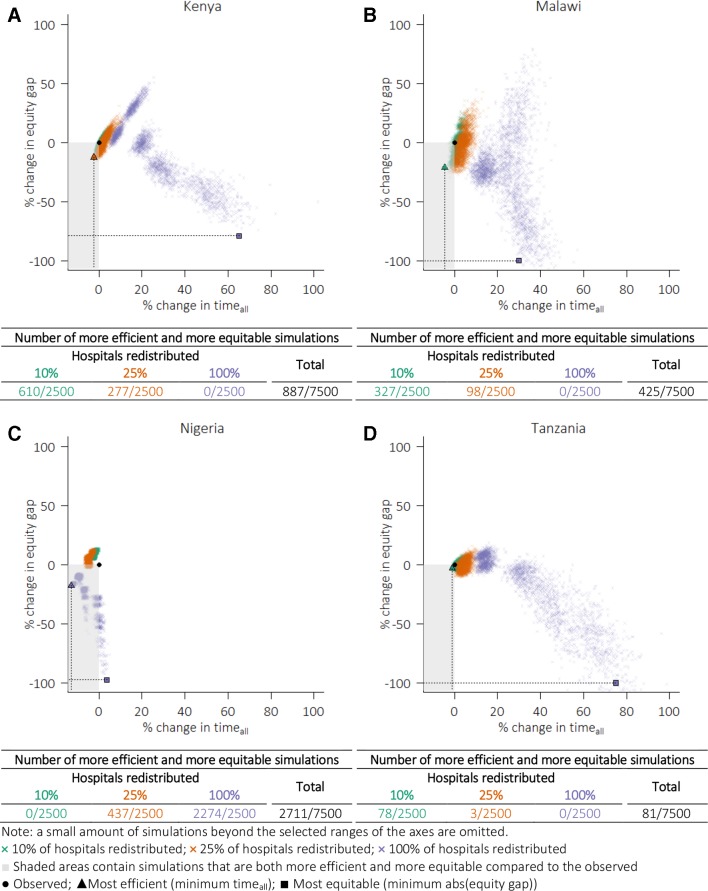
Having hospitals located in urban areas where people, resources and wealth concentrate is efficient, but leaves long travel times for the rural and often poorer population and goes against the equity objective. We aimed to assess the current efficiency (mean travel time in the whole population) and equity (difference in travel time between the poorest and least poor deciles) of hospital care provision in four sub-Saharan African countries, and to compare them against their theoretical optima.
We overlaid the locations of 480, 115, 3787 and 256 hospitals in Kenya, Malawi, Nigeria and Tanzania, respectively, with high-resolution maps of travel time, population and wealth to estimate current efficiency and equity. To identify the potential optima, we simulated 7500 sets of hospitals locations based on various population and wealth weightings and percentage reallocations for each country.
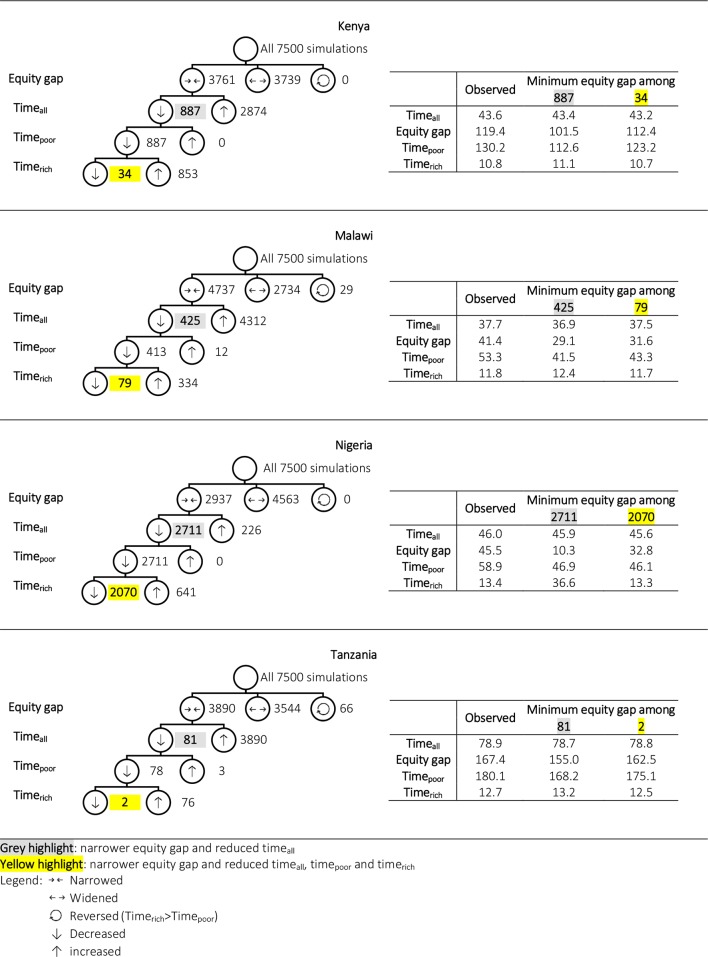
The average travel time ranged from 38 to 79 min across countries, and the respective optima were mildly shorter (<15%). The observed equity gaps were wider than their optima. Compared with the best case scenarios, differences in the equity gaps varied from 7% in Tanzania to 77% in Nigeria. In Kenya, Malawi and Tanzania, narrower equity gaps without increasing average travel time were seen from simulations that held 75%-90% of hospitals at their current locations.
Current hospital distribution in the four sub-Saharan African countries could be considered efficient. Simultaneous gains in efficiency and equity do not necessarily require a fundamental redesign of the healthcare system. Our analytical approach is readily extendible to aid decision support in adding and upgrading existing hospitals.
医院集中在人员、资源和财富密集的城市地区虽有效率,但农村地区(往往是较贫困人群)就医路途时间长,有悖公平目标。我们旨在评估撒哈拉以南非洲四个国家医院医疗服务提供的当前效率(全体人口的平均就医时间)和公平性(最贫困与最不贫困十分位数人群就医时间差异),并将其与理论最优值进行比较。
我们分别将肯尼亚、马拉维、尼日利亚和坦桑尼亚的480家、115家、3787家和256家医院的位置与高分辨率的出行时间、人口和财富地图叠加,以估计当前的效率和公平性。为确定潜在最优值,我们基于各国不同的人口和财富权重以及百分比重新分配情况,模拟了7500组医院位置。
各国平均就医时间在38至79分钟之间,各自的最优值略短(<15%)。观察到的公平差距比最优值更大。与最佳情况相比,公平差距的差异在坦桑尼亚为7%,在尼日利亚为77%。在肯尼亚、马拉维和坦桑尼亚,通过将75% - 90%的医院保持在当前位置的模拟发现,在不增加平均就医时间的情况下,公平差距缩小。
撒哈拉以南非洲这四个国家当前的医院分布可被认为是有效率的。效率和公平性的同时提升不一定需要对医疗系统进行根本性重新设计。我们的分析方法易于扩展,以辅助在增设和升级现有医院方面的决策支持。