Chen Yi-Lin, Lin Chien-Chung, Yang Shu-Ching, Chen Wan-Li, Chen Jian-Rong, Hou Yi-Hsin, Lu Cheng-Chan, Chow Nan-Haw, Su Wu-Chou, Ho Chung-Liang
Molecular Diagnosis Laboratory, Department of Pathology, National Cheng Kung University Hospital, Tainan, Taiwan.
Molecular Medicine Core Laboratory, Research Center of Clinical Medicine, National Cheng Kung University Hospital, Tainan, Taiwan.
Front Oncol. 2019 Jul 16;9:631. doi: 10.3389/fonc.2019.00631. eCollection 2019.
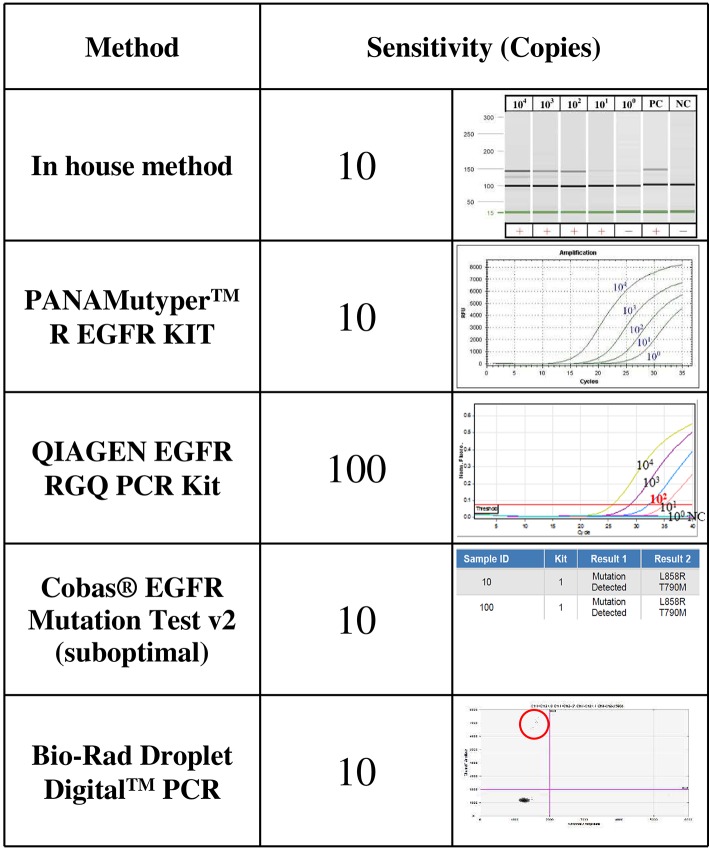
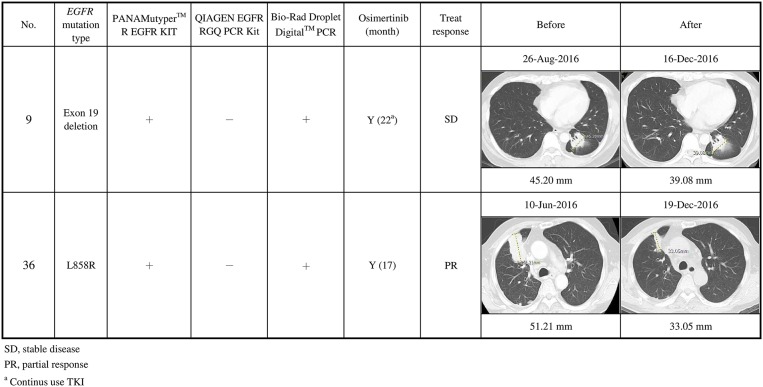
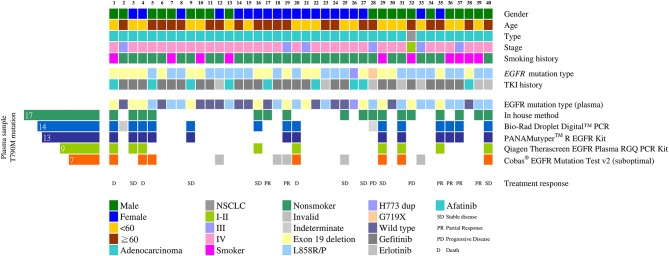
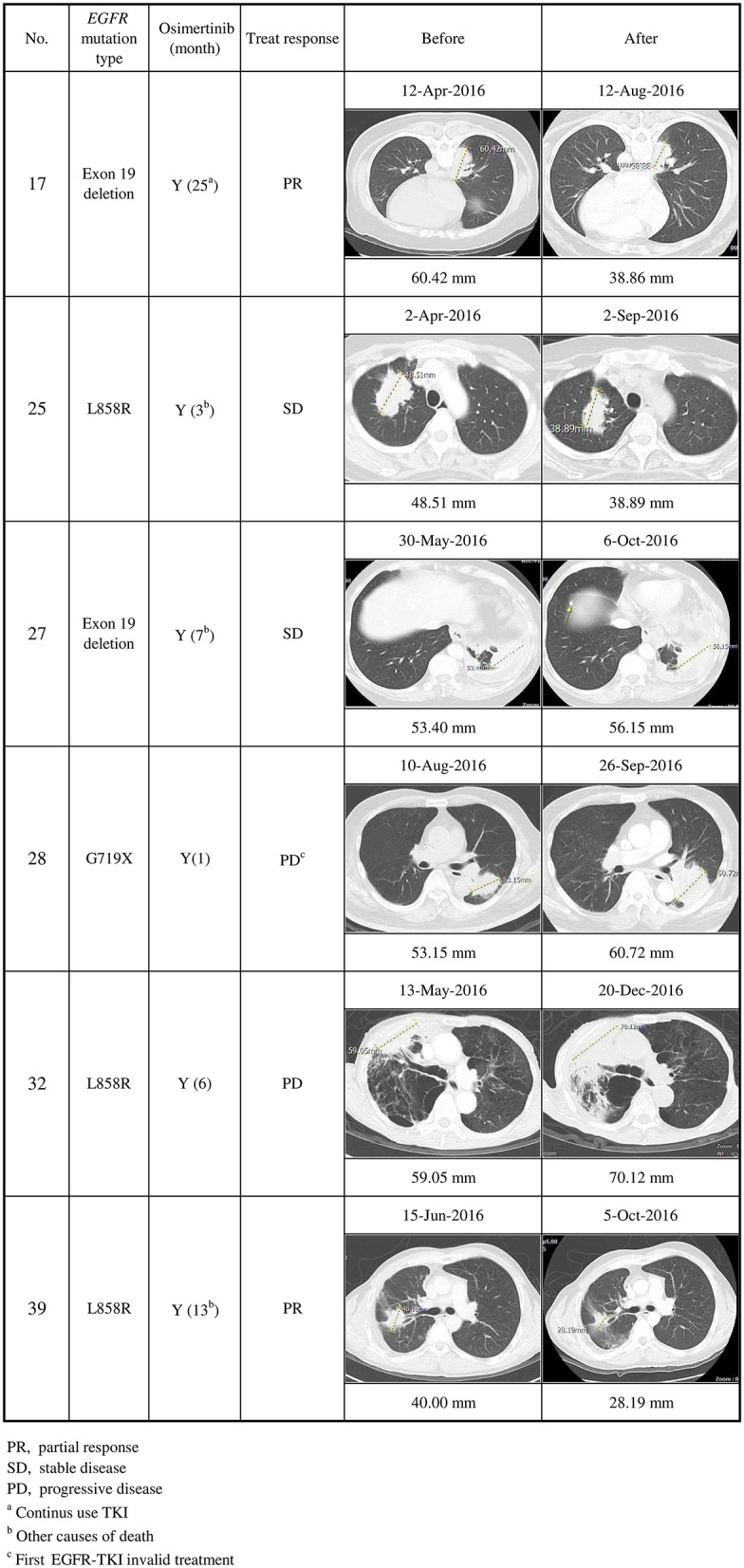
Third-generation tyrosine kinase inhibitors (TKIs) were developed to overcome T790M-mediated resistance to earlier generations of epidermal growth factor receptor -targeted TKIs. We compared four well-established and one in-house method for the analysis of the T790M mutation in plasma cell-free DNA (cfDNA), in hope to find a better way to select non-small cell lung cancer (NSCLC) patients appropriate for 3rd-generation TKI therapy. For sensitivity levels of each method, plasmid DNA with T790M mutations was serially diluted with cfDNA from healthy controls with wild type . The clinical performance was analyzed in a clinical cohort of mutation-positive NSCLC patients with acquired EGFR TKI resistance ( = 40). All methods except the therascreen kit (Qiagen) had a sensitivity level of 10 copies of T790M plasmid DNA in the spiked specimen. The detection rates of the T790M mutation in plasma cfDNA from the clinical cohort were 42.5, 35, 32.5, 22.5, and 17.5% for the in-house ARMS method, Bio-Rad droplet digital PCR, PANAMutyper, RGQ PCR Kit and Cobas EGFR Mutation kit (with suboptimal template amounts), respectively. Osimertinib was given to 17 of 20 patients with T790M mutations. The best treatment responses, based on the RECIST criteria, included 6 partial responses (PR) and 7 stable diseases (SD). The PANAMutyper and the Bio-Rad droplet digital PCR were comparable, the Cobas EGFR Mutation kit required significantly more template for testing. The best combination would be the in-house ARMS method plus the PANAMutyper or Bio-Rad droplet digital PCR, which would have a detection rate of 50% (20/40) and a disease control rate of 76% (13/17).
第三代酪氨酸激酶抑制剂(TKIs)的研发是为了克服T790M介导的对早期几代表皮生长因子受体靶向TKIs的耐药性。我们比较了四种成熟方法和一种内部方法,用于分析游离血浆DNA(cfDNA)中的T790M突变,希望找到一种更好的方法来选择适合第三代TKI治疗的非小细胞肺癌(NSCLC)患者。对于每种方法的灵敏度水平,将含有T790M突变的质粒DNA与来自野生型健康对照的cfDNA进行系列稀释。在一组40例获得性EGFR TKI耐药的T790M突变阳性NSCLC患者的临床队列中分析临床性能。除了therascreen试剂盒(Qiagen)外,所有方法在加标样本中对T790M质粒DNA的灵敏度水平均为10拷贝。临床队列中血浆cfDNA中T790M突变的检测率,内部ARMS方法、Bio-Rad液滴数字PCR、PANAMutyper、RGQ PCR试剂盒和Cobas EGFR突变试剂盒(模板量未达最佳)分别为42.5%、35%、32.5%、22.5%和17.5%。20例T790M突变患者中有17例接受了奥希替尼治疗。根据RECIST标准,最佳治疗反应包括6例部分缓解(PR)和7例疾病稳定(SD)。PANAMutyper和Bio-Rad液滴数字PCR相当,Cobas EGFR突变试剂盒检测所需的模板量明显更多。最佳组合是内部ARMS方法加PANAMutyper或Bio-Rad液滴数字PCR,其检测率为50%(20/40),疾病控制率为76%(13/17)。